
![]()
The Pyramid Dressing
A forgotten technique for focused haemorrhage control
An 18-year-old man is brought to the emergency department after punching through a glass window during an altercation.
On arrival, the paramedics observed a deep laceration over the medial aspect of the upper arm with brisk pulsatile bleeding. A tourniquet was applied proximal to the bleeding site and external haemorrhage controlled.
On arrival the patient is pale, diaphoretic and anxious.
- HR 128 bpm
- BP 102/64 mmHg
- Approximate tourniquet time: 45 minutes
- No palpable radial pulse distal to the inflated tourniquet
- The hand is cool, but clinically viable
The problem
The tourniquet has stopped the bleeding, but has also stopped distal perfusion.
- Releasing the tourniquet risks further arterial haemorrhage.
- Leaving it in place risks progressive limb ischaemia.
The challenge is to convert proximal tourniquet control into local haemorrhage control while restoring distal blood flow.

Pressure dressing solution?
The common response to ongoing bleeding is to add more gauze and wrap the bandage tighter.
That often fails for two reasons.
- Pressure is spread across a broad surface rather than concentrated over the bleeding vessel. The dressing may look impressive, but the vessel continues to bleed underneath it.
- Tight circumferential wrapping may further impair venous return and arterial inflow resulting in worsening distal ischaemia.
The primary principle is not simply “more pressure”…but pressure in the right place.
The pyramid dressing principle
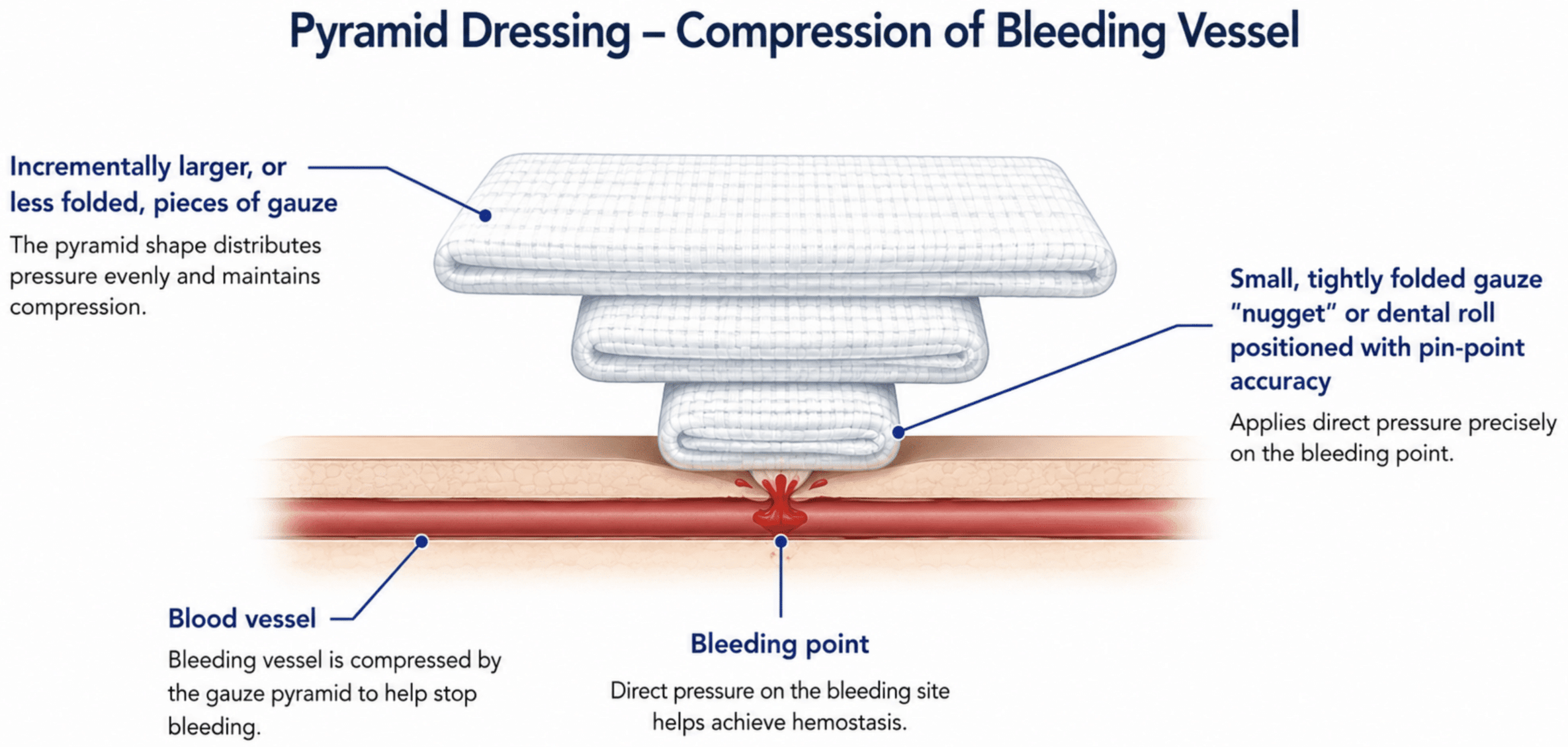
The pyramid dressing, also known as the “nugget technique”, converts broad external compression into focused pressure directly over the bleeding point. The principle is simple:
A small, firm gauze “nugget” placed directly over the bleeding vessel concentrates force onto a small area. Progressively larger layers of gauze are then placed above it, creating an inverted pyramid. The upper layers stabilise the nugget and distribute the securing force, while the smallest layer delivers focused pressure to the vessel.
The technique is not a definitive vascular repair. It is a temporising bridge to theatre, interventional radiology or surgical haemorrhage control.
When to consider a pyramid dressing?
Consider a pyramid dressing when there is severe external haemorrhage from a compressible limb wound and the bleeding point can be localised.
The pyramid dressing is particularly useful when a tourniquet has controlled haemorrhage but continued tourniquet inflation threatens distal perfusion.
Do not use the technique to delay definitive care. Do not blindly probe deep wounds. If bleeding cannot be localised or controlled quickly, reapply the tourniquet and escalate.
How to perform a pyramid dressing
1. Prepare before releasing the tourniquet
Keep proximal haemorrhage control in place while the team prepares. Have ready:
- sterile gauze
- haemostatic gauze, if available
- a compression bandage
- suction and good lighting
- immediate ability to re-tighten the tourniquet
Warn the team before loosening the tourniquet.
2. Expose and identify the bleeding point
Carefully expose the wound.
Slowly loosen the tourniquet only enough to identify the bleeding point. If brisk bleeding recurs, apply direct finger pressure immediately.
The finger is not a dressing. It is a temporary marker and haemorrhage-control device while the dressing is built.
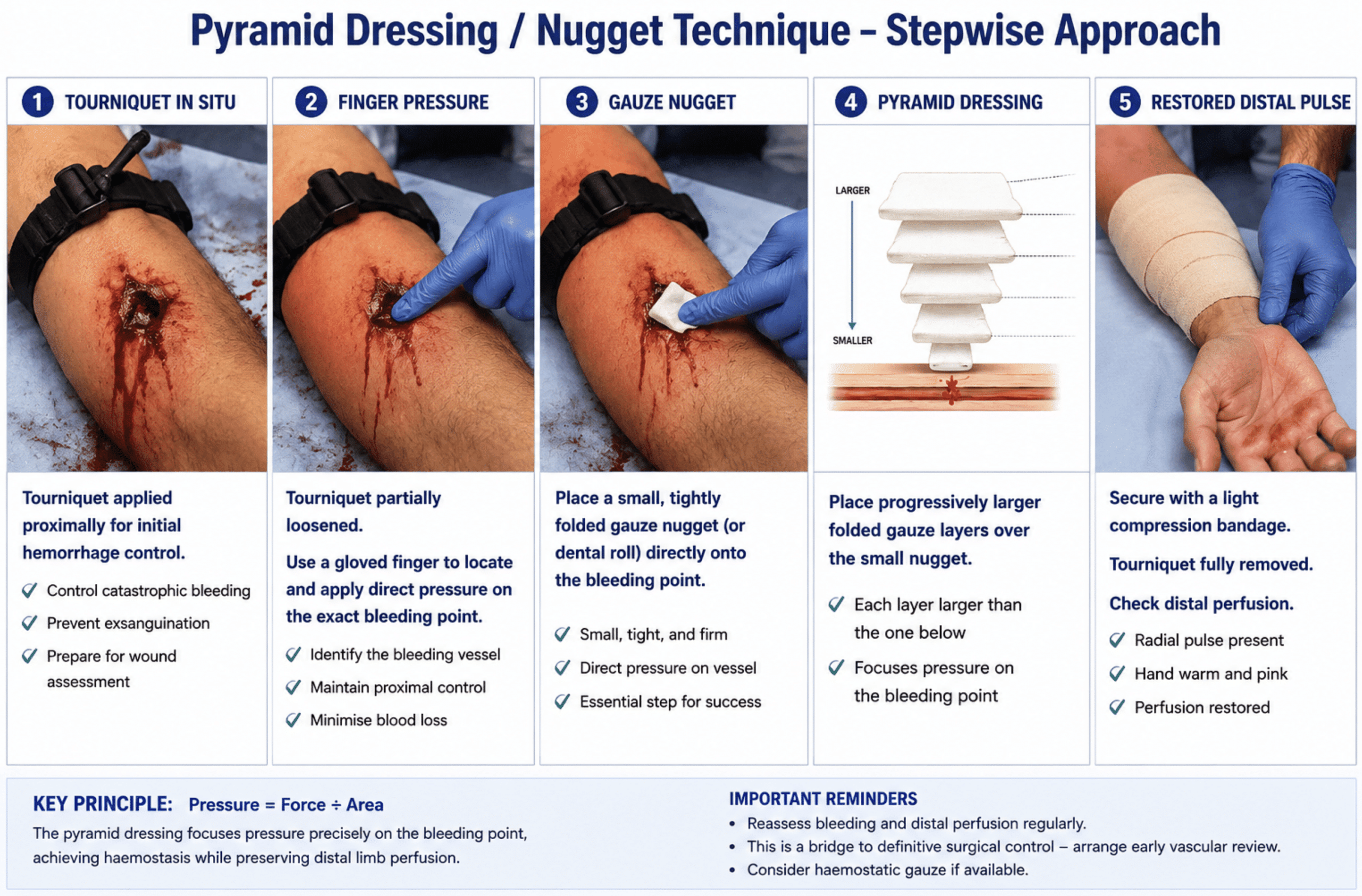
3. Place the nugget
Replace the finger with a small, tightly folded gauze nugget or dental roll positioned precisely over the arterial defect.
This is the critical step.
The nugget must sit directly on the bleeding point. If it is off-target, the rest of the dressing will fail no matter how tightly it is wrapped.
Haemostatic gauze may be used for the nugget when available.
4. Build the pyramid
Place progressively larger folded gauze layers over the nugget.
Each layer should be wider than the one below it. The small lower layer focuses pressure; the broader upper layers stabilise the dressing and prevent the pressure point from shifting.
5. Secure without strangling the limb
Secure the dressing with a compression bandage.
The aim is focused pressure, not maximal circumferential compression. A well-built pyramid dressing should control the bleeding without needing to occlude the entire limb.
After securing the dressing, reassess:
- bleeding through the dressing
- radial/ulnar pulse
- capillary refill
- skin temperature and colour
- motor and sensory function
- pain out of proportion
If haemorrhage recurs, reapply direct pressure, re-tighten the tourniquet if required, and escalate.
Back to the case
The trauma team prepared gauze, haemostatic dressing and a compression bandage before loosening the tourniquet.
As the tourniquet was gradually released, bright arterial bleeding recurred from a small defect in the brachial artery. Direct finger pressure was applied immediately. A tightly folded gauze nugget was placed precisely over the bleeding point, followed by three progressively larger layers of folded gauze. The dressing was secured with a light compression bandage.
The tourniquet was removed. The dressing remained dry, the radial pulse returned, and the hand became warm and well perfused.
The patient proceeded to theatre, where vascular surgery repaired a partial brachial artery laceration.
Take-home points
- The tourniquet buys time but is not definitive treatment.
- Do not release a tourniquet until the team is ready.
- Identify the exact bleeding point.
- Use a small, firm gauze nugget directly over the vessel.
- Build progressively larger layers above it.
- Avoid excessive circumferential compression.
- Reassess distal perfusion repeatedly.
- Use haemostatic gauze when available.
- Treat the pyramid dressing as a bridge to definitive haemorrhage control, not a substitute for vascular repair.
The pyramid dressing solves a mechanical problem converting broad, limb-threatening compression into focused haemostasis directly at the bleeding vessel.
References
- Shokrollahi K, Sharma H, Gakhar H. A technique for temporary control of hemorrhage. J Emerg Med. 2008 Apr;34(3):319-20.
- Nickson C. Trauma! Extremity Arterial Haemorrhage. LITFL
Emergency Procedures
Emergency nurse with ultra-keen interest in the realms of toxicology, sepsis, eLearning and the management of critical care in the Emergency Department | LinkedIn |