
![]()
Theophylline toxicity
It is well known that theophylline has a narrow therapeutic index, hence it will be extremely rare that you find a patient on this drug and also its absence from most status asthmaticus guidelines with the exception of paediatrics. Both acute and chronic overdose is potentially life-threatening requiring aggressive supportive care and dialysis to ensure a good outcome. Aminophylline is the the water-soluble complex of theophylline that is used for IV. It rapidly dissociates in vivo to release theophylline.
Toxic Mechanism:
Multiple mechanisms have been proposed including antagonism of adenosine, altered intracellular calcium transport and elevated cAMP concentration. All these mechanisms combined result in metabolic abnormalities, cardiac dysrhythmias and seizures.
Toxicokinetics:
- Good oral absorption but is delayed with modified release preparations with peak levels not occurring until 15 hours post ingestion.
- Rapidly distributed with a volume of distribution of 0.5 L/kg
- Metabolised in the liver which is variable and saturable.
- Elimination half-life is prolonged in overdose.
Resuscitation:
- Seizures: Benzodiazepines (varying doses in the textbooks, easy method is 0.1mg/kg IV for lorazepam (max 4mg) / midazolam (max 10mg) / diazepam (max 10mg). Or…
- Lorazepam 0.1mg/kg max 4mg
- Diazepam 0.15mg/kg max 10mg
- Midazolam 0.2mg/kg max 10mg
- Hypotension: Give 10 – 20 ml/kg of IV crystalloid, if response is not adequate start noradrenaline dose: 0.15mg/kg in 50ml D5W at 1-10ml/hr (0.05 – 0.5 mcg/kg/min)
- Ventricular and supra ventricular tachycardia: carefully titrate beta blockers (beware of bronchospasm in susceptible individuals).
- Propranolol 0.5 – 1 mg IV every 5 minutes
- Metoprolol 5mg (0.1 mg/kg in children) IV every 5 minutes
- Esmolol 0.05 mg/kg/minute and titrate to response. More selective and better tolerated in asthmatics.
Risk Assessment
- Dose-related risk assessment for an acute ingestion:
- 5 – 10 mg/kg = therapeutic loading dose
- >10 mg/kg = Potential toxicity
- >50 mg/kg = Life threatening toxicity
- Patients with chronic toxicity usually have a poorer outcome as the diagnosis is often overlooked and they are often elderly with other co-morbidities. They usually present with vomiting and tachycardia, seizures or dysrhythmias maybe present.
- Serum theophylline levels will help further refine the risk assessment.
- Anyone who is suspected of developing toxicity needs to be in a centre where haemodialysis or charcoal haemoperfusion can be given. With modified-release preparations there is a delay of many hours before deterioration occurs.
- Children: One 200 mg modified release tablet will produce toxicity in a 10 kg toddler. Ingestion of multiple tablets can be life-threatening.
- Clinical features:
- Early: anxiety, vomiting, tremor and tachycardia
- Severe poisoning indicating poor prognosis: SVT, AF, flutter, VT, refractory hypotension, seizures.
- Metabolic abnormalities: Severity is worse with acute ingestions compared to chronic toxicity. Hypokalaemia (can be refractory), hypophosphataemia, hypomagnesaemia, hyperglycaemia, metabolic acidosis.
Supportive Care
- Correct electrolyte abnormalities
- Treat vomiting with antiemetics
- If intubated see FASTHUGSINBED for further supportive care.
Investigations
- Screening: 12 lead ECG, BSL, Paracetamol level
- Specific:
- Arterial blood gas, EUC, Magnesium, Phosphate, Calcium
- Theophylline levels – correlate well with clinical severity and are repeated every 2 – 4 hours until falling.
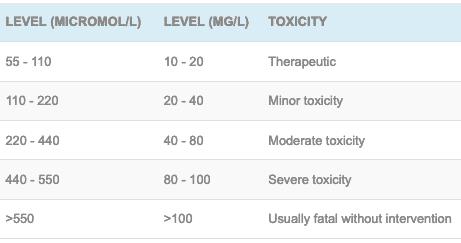
- In the elderly and those with chronic toxicity severe intoxication can occur at the ‘moderate toxicity’ level >60 mg/L and >40 mg/L retrospectively.
Decontamination:
- Activated charcoal 50 grams (1 g/kg in children) can be given following an acute overdose even if delayed. The risk of aspiration will need to be considered if the patient is seizing and dialysis prioritized.
Enhanced Elimination
- Haemodialysis (if possible charcoal haemoperfusion is the modality of choice).
- Indications for dialysis include:
- Theophylline level >550 micromol/L (100 mg/L) with acute overdose
- Theophylline level >330 micromol/L (60 mg/L) with chronic toxicity
- Clinical manifestation of severe toxicity – dysrhythmia, hypotension or seizures.
- Multi-dose activated charcoal can be used but often delays haemodialysis.
Antidotes
- None available
Disposition
- Patients who have ingested the syrup and are well at 6 hours post ingestion are medically cleared.
- Overdose of modified-release preparations requires a 12 hour period of observation although serial theophylline levels may speed this process up.
- All symptomatic patients require HDU setting, if there are progressive clinical features, rising levels indicating severe toxicity or a risk assessment that would indicate severe toxicity is likely the patient needs to be in a centre capable of enhanced elimination as described above.
References and Additional Resources:
Additional Resources:
- Tox conundrum 014 – Theophylline overdose
- CCC – Theophylline
References:
- Minton NA and Henry JA. Treatment of theophylline overdose. American Journal of Emergency Medicine 1996;14:606-612.
- Shannon M. Life-threatening events after theophylline overdose: a 10-year prospective analysis. Archives of Internal Medicine 1999;159:989-994.

Toxicology Library
DRUGS and TOXICANTS
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.