
![]()
Ultrasound Case 044
Presentation
A 51 year old man with known gallstones presents feeling unwell with some dull epigastric ache, dark urine and pale stool.
Could it be choledocholithiaisis?
View 2

View 3
View 4

Describe and interpret these scans
IMAGE INTERPRETATION
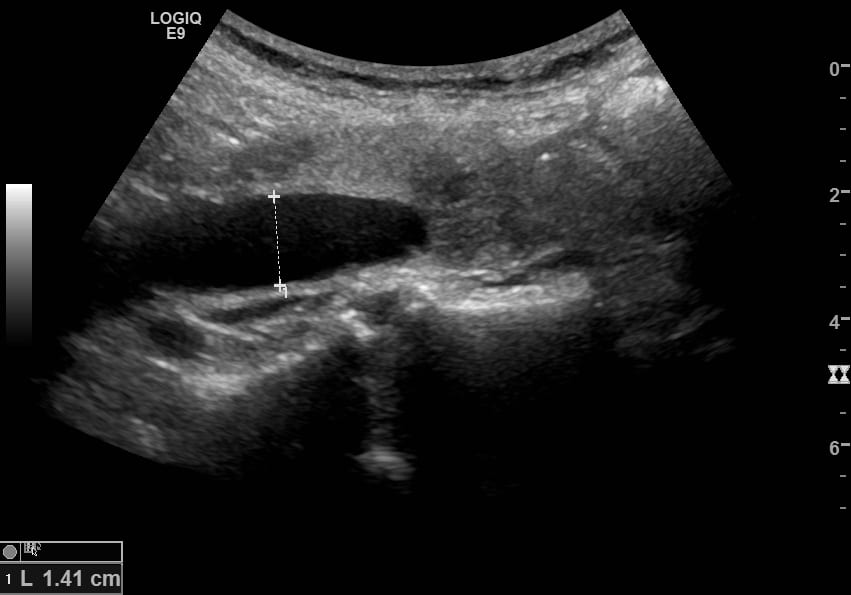
Image 1: Transverse epigastric view fanning through the pancreas from superior to inferior.
The first abnormality one sees is the very dilated common bile duct (CBD). It is almost the same size as the aorta, and in this view you are viewing it transversely. As you fan down you see a rounded hypoechoic lymph node lying between the CBD and aorta. Then the CBD abruptly stops and a mass is seen in the head of the pancreas. It is relatively hypoechoic but solid.

Image 2: Gallbladder. The thin walled slightly distended gallbladder contains a large stone toward the neck and some dependent sludge. Deep to it is a rounded para aortic lymph node.
Image 3: Distal CBD in longitudinal section. The CBD is markedly dilated at 14mm (≤6mm in this age group). It can be seen to gradually taper before abruptly stopping. Normal pancreatic tissue is seen above it as homogeneous mid echogenic tissue. The more hypoechoic slightly coarser echo textured mass obstructing the duct is tumour. No CBD stone is present.
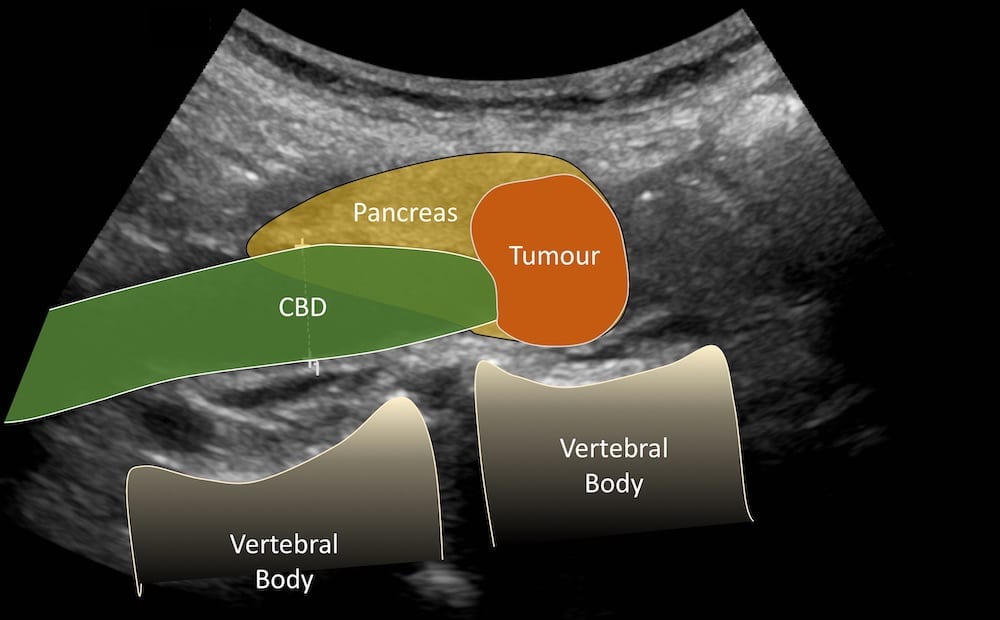
Image 4: Transverse view of the right lobe of the liver. There are multiple poorly defined heterogeneous lesions distorting the normal liver architecture. These are metastases.
CLINICAL CORRELATION
Obstructive jaundice with pancreatic head tumour and liver metastases
An orderly technique is important in your approach to obstructive jaundice, or pathology will be missed.
Pancreas: I begin with the pancreas, imaging the head, body and tail in two planes. Measure the pancreatic duct if dilated, measure any focal abnormality. Look for para aortic lymphadenopathy.
Distal CBD: Find the distal CBD in the posterior part of the pancreatic head. It initially runs cranially and then turns toward the right shoulder. Trace it carefully searching for the cause of obstruction. In western society the most common intraluminal cause of obstruction is stones and sludge, and extraluminal cause malignancy of the pancreatic head, most usually pancreatic adenocarcinoma.
Left and then right lobe of liver: Imaged in two planes, looking for intrahepatic duct dilation, tumour either primary or metastatic, or other abnormality. Again measure and document any abnormality noted.
Gallbladder: Imaged in two planes. Measure and characterize the GB wall thickness against the liver where it is most easily defined, and the measure the GB diameter if enlarged. Note GB content including stones or sludge, particularly noting any stones in the neck or cystic duct, and if they are mobile. Note tenderness to probe pressure. Now the mid and proximal CBD are examined and measured searching again for stones or extrinsic compression.
Positioning: Rolling the patient onto their left side can assist if imaging has not been ideal.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |