
![]()
Ultrasound Case 046
Presentation
A 22 year old woman presents with very mild pelvic discomfort and vomiting in early pregnancy. She has had a previous ectopic pregnancy and is worried this may be an ectopic pregnancy.
You perform a transabdominal pelvis scan.
Describe and interpret these scans
IMAGE INTERPRETATION
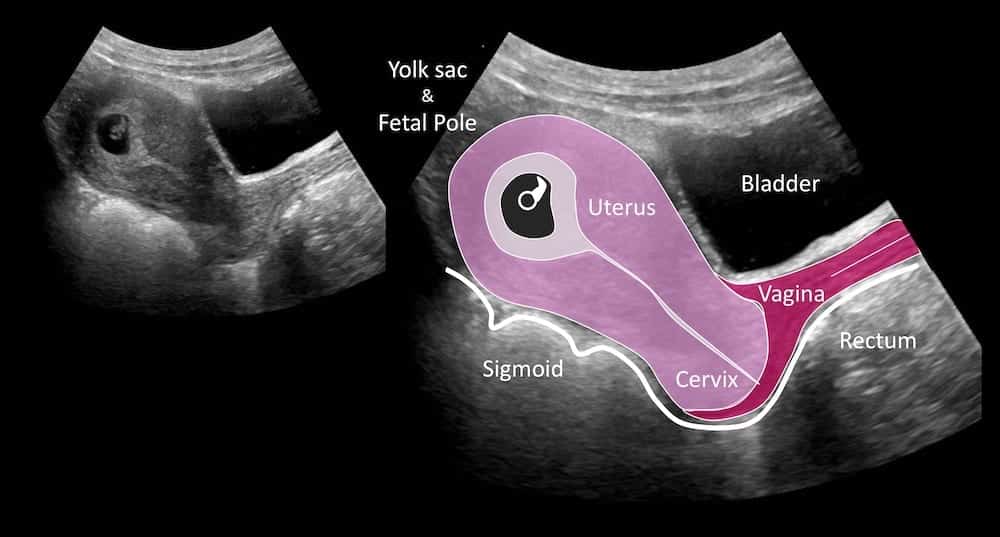
Image 1: Longitudinal view of the uterus, cervix and vagina, then zoomed in image of gestation sac.
Image 2: Key to image 1.
CLINICAL CORRELATION
Single live intrauterine pregnancy (SLIUP) at 6 weeks gestation.
In scanning an early pregnancy there are several essential steps.
- Scan the entire pelvis in transverse from superior to inferior and vice versa; then scan in longitudinal from one side of the pelvis to the other. Ideally a full bladder will aid in providing an acoustic window through which the uterus and ovaries can be seen – although even with an empty bladder reasonable views are frequently possible.
- Find the uterus and be sure what you are looking at is the uterus – you need to be able to follow it to cervix and vagina – occasionally an ectopic can be surrounded by blood clot and look like the uterine fundus.
Assess for free fluid and blood clot in the Pouch of Douglas and beyond.
Assess the uterine cavity for a gestation sac. Measure it and consider its position in the uterus. It should sit centrally within the fundus. Remember an interstitial ectopic lies within the interstitial portion of the Fallopian tube where it traverses the myometrium. Also a scar ectopic lies in the anterior lower uterine segment at the site of a previous C-section scar, and a cervical ectopic lies within the cervix. Get expert advice if you’re not sure.
Search for evidence that the sac you are looking at it is a definite pregnancy – it contains a yolk sac and / or a fetal pole. Measure the crown rump length (CRL) and work out a gestational age.
Assess for viability by watching for the embryonic cardiac activity. It is first evident on transvaginal scan at about 5 weeks and 5 days. It begins as a subtle flicker at about 100 beat per minute, and increases to between 120 and 160 by 7 weeks.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |
