
![]()
Ultrasound Case 064
Presentation
A 15 year old boy has had vomiting and diarrhoea for 2 days. He has developed increasing right iliac fossa pain which has suddenly increased and is colicky in nature.
View 2
View 3-5


View 6-7
View 8
Describe and interpret these scans
IMAGE INTERPRETATION
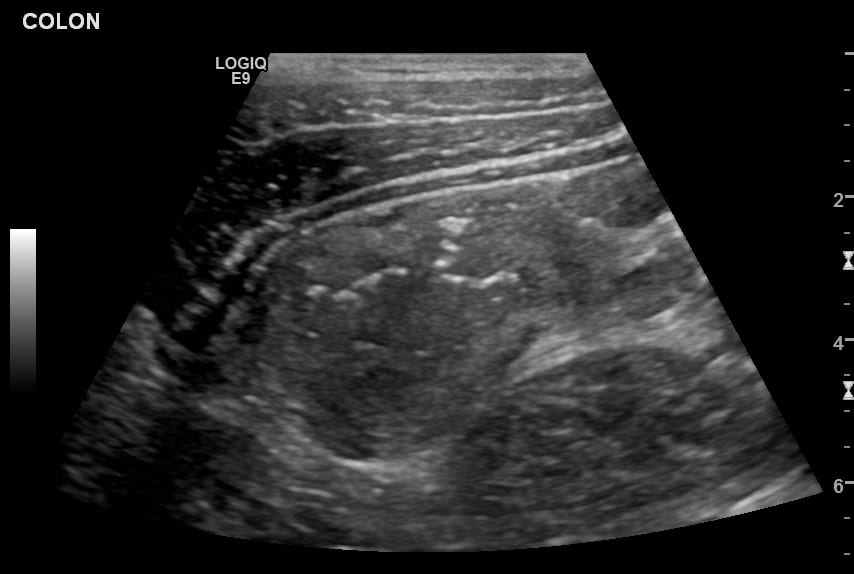
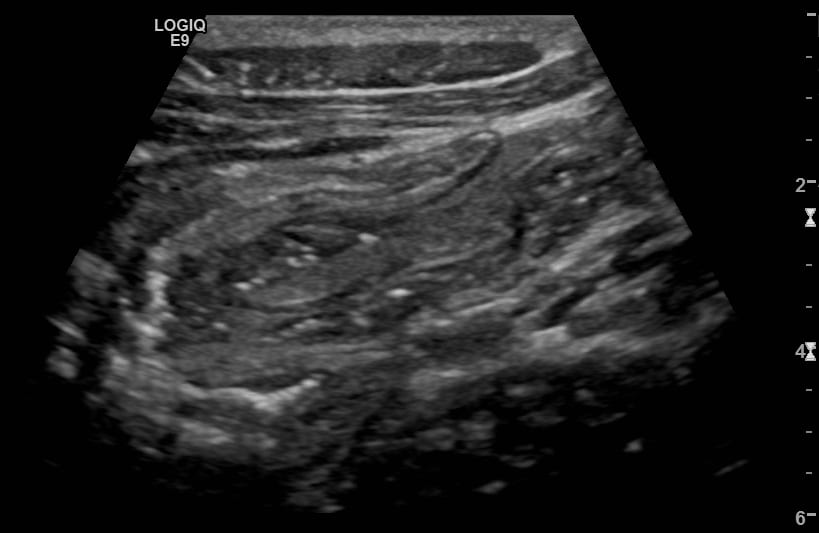
Image 1 & 2: Transverse view, sweeping the transducer inferolaterally in the right iliac fossa.
Several enlarged mesenteric lymph nodes are seen.
The mesenteric fat is relatively echogenic indicating some inflammatory change.
The caecum / ascending colon is markedly thickened.
A short segment of ileoileal intussusception is present. This has the appearance of a rounded targetoid mass with concentric hyper and hypoechoic rings when viewed in transverse section. There is a thin inner fat core with little mesenteric fat having been dragged into the intussusception – this tends to be the pattern of small bowel intussusception rather that ileocolic intussusception where more mesenteric fat enters the intussusceptum, creating a larger often asymmetrical echobright focus – the pseudokidney appearance.
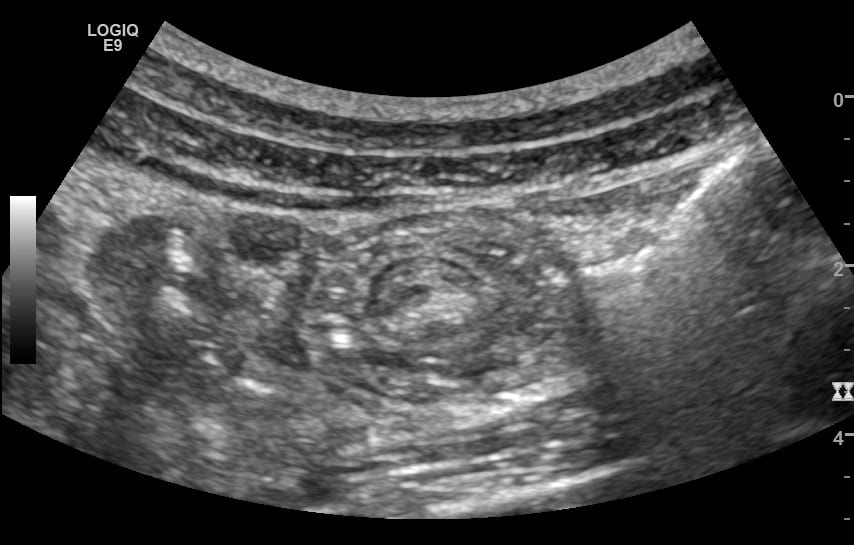
Images 3-5 Transverse views showing the markedly thickened caecum and ascending colon.
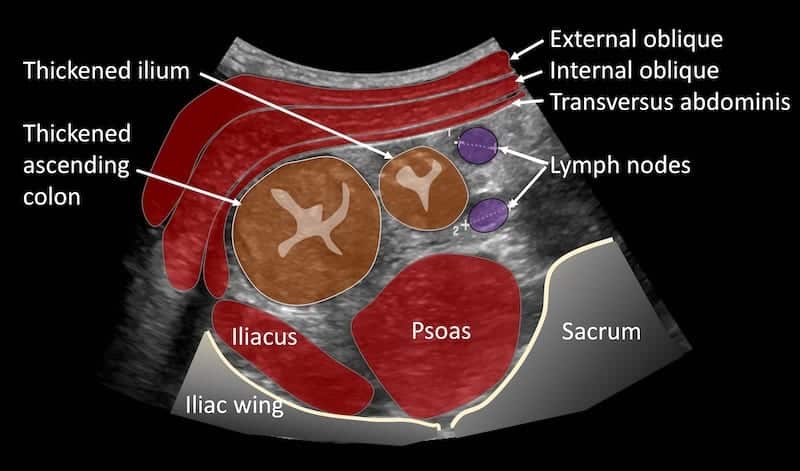
Image 6 & 7: Long and short axis views of the ileoileal intussusception.


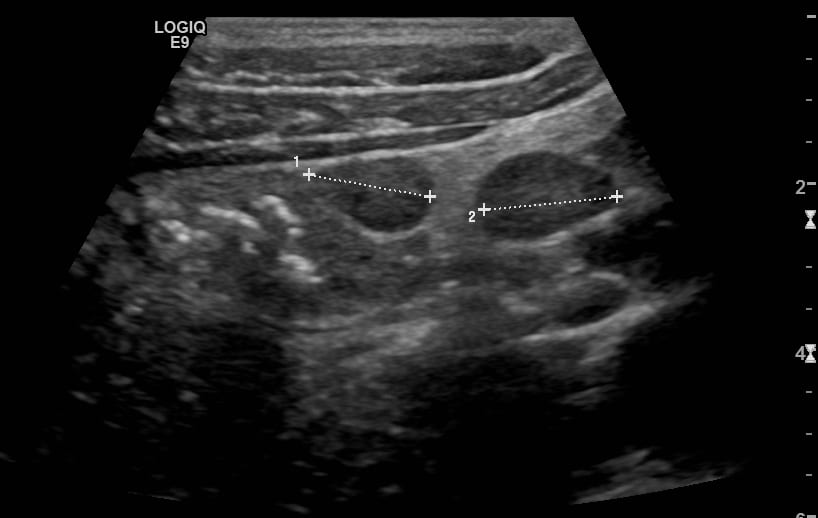
Image 8: Mesenteric lymph nodes and echogenic mesenteric fat.
CLINICAL CORRELATION
Infectious enteritis and colitis with mesenteric lymphadenopathy and ileoileal intussusception
This young man had the typical clinical features of an infectious gastroenteritis – until he developed right iliac fossa pain.
I was asked to assess for appendicitis and / or mesenteric adenitis.
Thickening of the ileum and ascending colon wall is quite common with infectious enteritis / colitis and Yersinia and Salmonella are organisms that have a particular predilection for these sites. Enteritis and colitis with associated mesenteric lymphadenopathy could have explained his RIF pain; but the short segment of intussusception is likely to have contributed further.
Small bowel intussusception (rather than ileocolic intussusception) often spontaneously reduces. In this case we carefully monitored the patient and the following morning his pain had substantially improved. Repeat ultrasound confirmed reduction in the intussusception.
Our hypothesis is that lymphoid hypertrophy of Peyer’s patches facilitated the intussusception.
Although his appendix was not visualised the inconsistent history and alternate explanation was reassuring. Other causes of thickened terminal ileum and caecum / ascending colon would include inflammatory bowel disease, typhlitis and malignancy, however clinical correlation and rapid resolution of symptoms enabled us to disregard a broader differential diagnosis.
There are several ways to sonographically differentiate small bowel from ileocolic intussusception. The presence of echogenic fatty tissue in the center of the intussusception is seen in patients with ileocolic intussusception. Conversely, small-bowel intussusception typically have a multilayered “double ring” appearance and demonstrated no or minimal linear echogenic fat tissue in the centre (as in this case)

REFERENCES
- Childers BC, Cater SW, Horton KM, Fishman EK, Johnson PT. CT Evaluation of Acute Enteritis and Colitis: Is It Infectious, Inflammatory, or Ischemic?RadioGraphics. 2015;35(7):1940-1941
- Lioubashevsky N, Hiller N, Rozovsky K, Segev L, Simanovsky N. Ileocolic versus small-bowel intussusception in children: can US enable reliable differentiation? Radiology. 2013 Oct;269(1):266-71.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |
