
![]()
Ultrasound Case 065
Presentation
A 24 year old male presents with 36 hours of right testicular pain. He is a poor historian and can’t provide details for the onset, although he has risk factors for sexually transmitted infection. His right testis is swollen and tender. The clinical question is torsion vs epididymo-orchitis.
View 2
View 3
View 4
View 5
View 6
Describe and interpret these scans
IMAGE INTERPRETATION
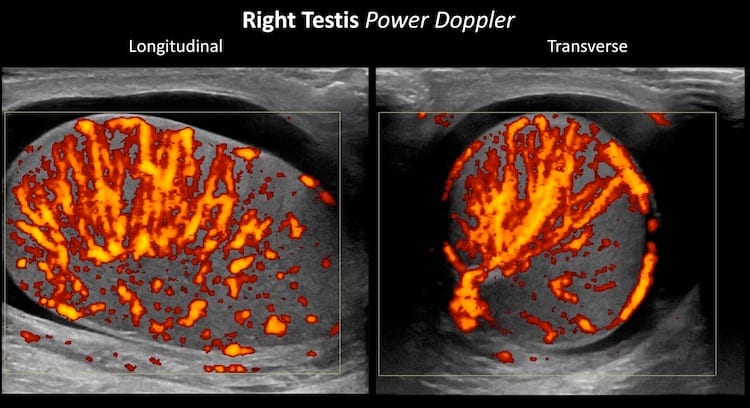
Image 1: Transverse view sweeping from superior to inferior through the right testis; Power Doppler. PARA Marked hypervascularity is evident. Views like this coined the term scrotal “inferno“.
Image 2: Longitudinal view sweeping across the testis. Again increased vascular flow is evident.
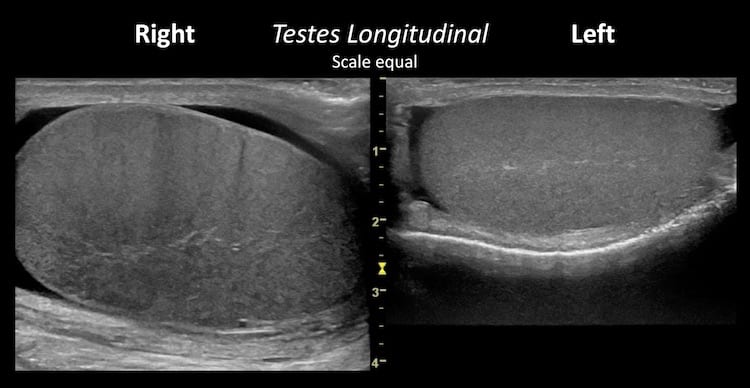
Image 3: Longitudinal views of both testes for comparison; the scale is the same. Grey scale or B-mode changes or orchitis can be subtle. Here there is:
- Scrotal wall thickening
- A small simple hydrocele.
- An enlarged and rounded right testis.
- Testicular echotexture is relatively hypoechoic and heterogenous on the right, with a subtle tigroid appearance caused by dilated testicular vasculature.
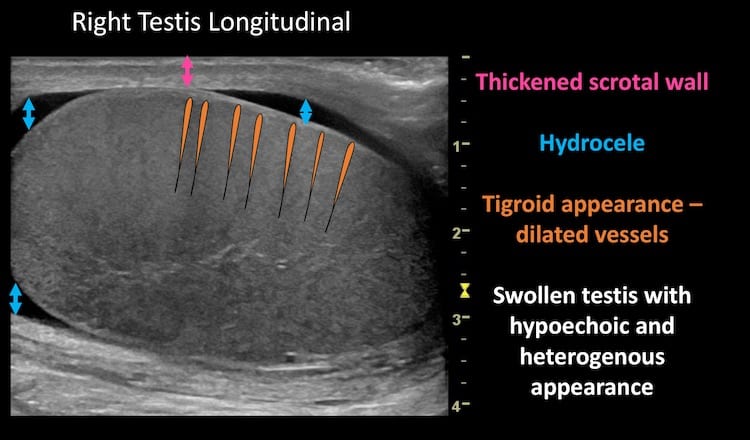
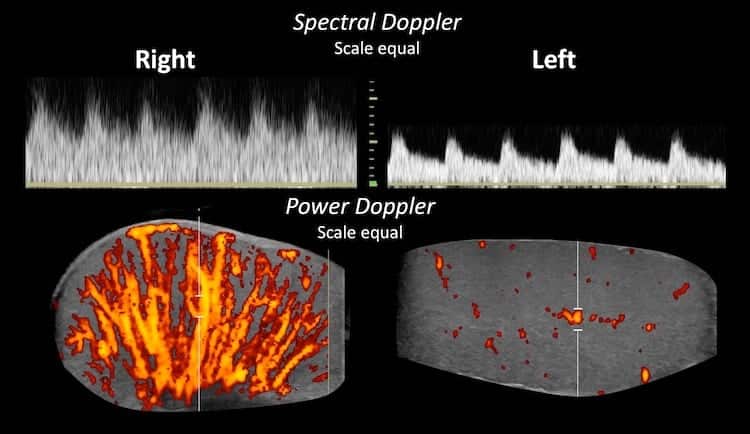
Image 4: Still longitudinal power Doppler images documenting the inferno of orchitis.
Image 5: Direct comparison of spectral Doppler examination of both testes with scales set identically. Both testes show a low resistance pattern of flow. Flow in the right testis has higher systolic and higher diastolic velocities than the normal left side. Calculation of the resistive index on the right (RI = (peak systolic velocity – end diastolic velocity)/peak systolic velocity) shows even lower resistance in the right testis which is not surprising – there is extreme vasodilation. RI Right = 0.40; RI Left = 0.58.
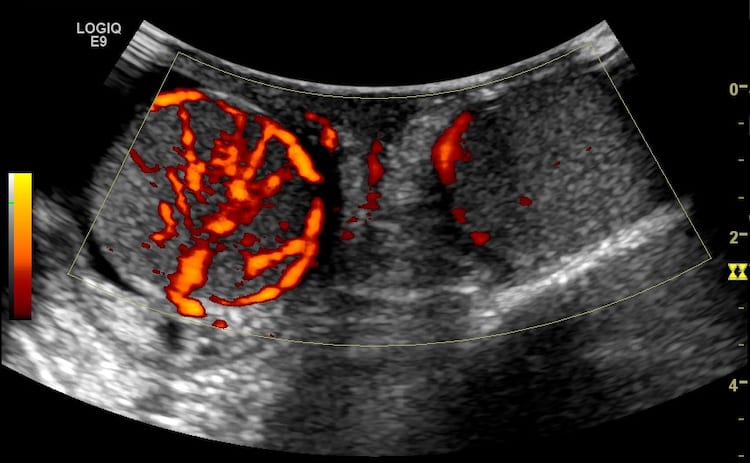
Image 6: The “spectacle” or “sunglasses” view – both testes are seen in transverse section in a single image – for comparison. The scrotal swelling meant this was best achieved with the curvilinear transducer, however resolution is poor. Never the less, the changes of hypervascularity in the right testis are again evident.
CLINICAL CORRELATION
Right epididymo-orchitis with scrotal “inferno“
Orchitis in this age group, with these risk factors is usually associated with epididymititis and termed epididymo-orchitis. This case had a slightly hyperaemic and inflamed right epididymis, but the testicular changes were more marked.
Very important points:
- Ultrasound should not delay urological opinion and if required operative intervention in suspected testicular torsion.
- The presence of testicular flow does not exclude torsion. It is not uncommon for some flow to remain despite ongoing torsion. Torsion – detorsion can occur and hypervascularity of the testis may be present reflecting a reperfusion hyperaemia.
- In severe orchitis testicular infarction may occur. These may be focal (often wedge-shaped) or generalised.
- Where not immediately evident, the diagnosis is made by carefully correlating the history, the examination and and sonographic findings and maintaining a high index of suspicion.
- The experience of the operator as well as the quality of the ultrasound machine and subsequent gray-scale and Doppler images makes a big difference in the acquisition and the interpretation of the images.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |