
![]()
Ultrasound Case 079
Presentation
A previously well 49 year old man presents with chest pain. He is tachycardic, tachypneoic and hypoxic with blood pressure 110/65. He is 2 weeks post ankle surgery.
View 2: Apical 4 chamber view.
Describe and interpret these scans
IMAGE INTERPRETATION
Image 1: Parasternal short axis cardiac view.
The right heart is dilated with little contraction during systole. The left heart is hyderdynamic with high ejection fraction.
Most obvious is the flattening of the interventricular septum – the “D-shaped” septum. But it’s not that simple. Watch very carefully and you will see paradoxical septal motion in early diastole and early systole.
Let’s start at the end of diastole. The septum is flat, both the RV and LV are as full as they will be but the low left sided pressures and volume combined with the abnormally high right sided pressures and volumes flatten the septum. As systole begins the pressure in the LV rises. The non-septal walls start to move inward but the septum initially paradoxically moves outward until the LV becomes circular. Then all walls contract together moving inward and keeping the LV cavity round in cross section. Then diastole begins. The non-septal LV walls relax and move outward lowering the LV pressure. The septum again moves paradoxically inward in early diastole until it is flattened, then as the LV fills the septum moves outwards in its flattened state.
This paradoxical early diastolic and early systolic septal movement reflects the acute fall in LV pressure and volume load compared to the acute rise in RV pressure and volume load.
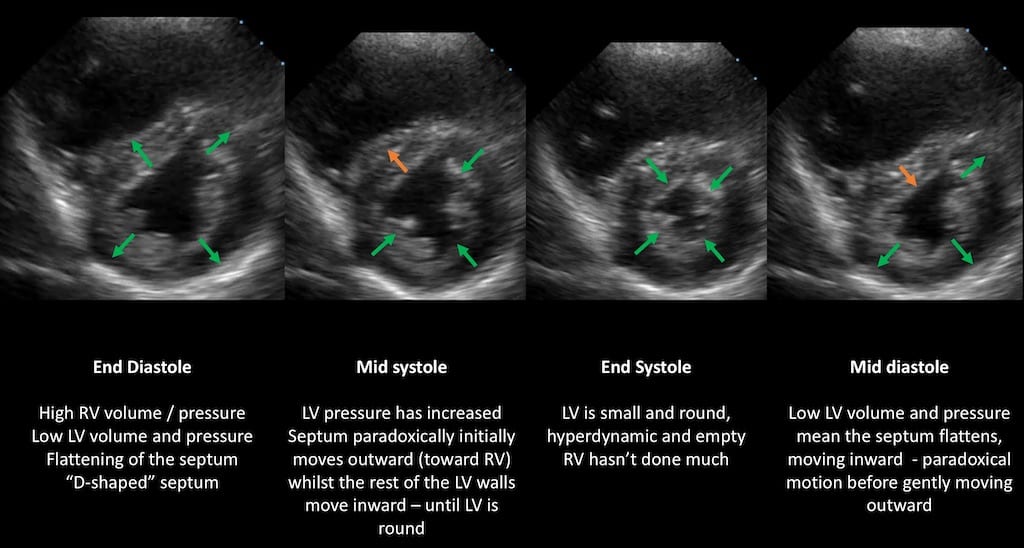
Image 2: Apical 4 chamber view.
The right ventricle is dilated – at least as big as the left ventricle in this view. RV function is reduced with TAPSE (tricuspid annular pan systolic excursion) measured at 15mm (≥16mm is normal). McConnell’s sign is present.

CLINICAL CORRELATION
Pulmonary embolism with McConnell’s sign and paradoxical septal motion and a D-shaped septum.
Clinically this is most probably a pulmonary embolism and you are looking for evidence to support this diagnosis. It’s probably a PE. Is there a DVT or PE in transit? Could it be chronic pulmonary hypertension – are there clues in the history, is the RV free wall trabeculated and thickened? Could it be an RV infarction? If he’s normotensive a CTPA is indicated and will confirm the diagnosis. If he deteriorates with hypotension or cardiac arrest you will need to manage it as a massive PE and consider thrombolysis immediately.
Remember unless you see thrombus in transit or sitting in pulmonary arteries, echo alone does not have adequate sensitivity or specificity to absolutely confirm or exclude PE. You must tie it in with clinical features and often other investigations to reach a definite conclusion.
McConnell’s sign is hypokinesis or akinesis of the mid right ventricular free wall, with preserved function or hyperkinesis of the RV apex. It was originally touted as highly sensitive (94%) and specific (77%) but more recent studies have been more conservative in their praise. MR studies have suggested the mechanism for McConnell’s sign is that the hyperdynamic, underfilled, hyperadrenergic LV apex pulls on the adjacent RV apical fibers giving the appearance of hyperkinesia of this region.
Right ventricular infarction and pulmonary hypertension have also both been associated with McConnell’s sign, hence the more recent hesitation in relying on this sign alone to make a diagnosis. Use as many diagnostic prompts as the clinical situation allows.
Reference:
McConnell MV, Solomon SD, Rayan ME, Come PC, Goldhaber SZ, Lee RT. Regional right ventricular dysfunction detected by echocardiography in acute pulmonary embolism. Am J Cardiol. 1996 Aug 15;78(4):469-73. [PMID 8752195]
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |