
![]()
Ultrasound Case 078
Presentation
A 48 year old woman presents with RUQ pain of 3 days duration. She has had several similar briefer episodes but on this occasion it has not settled and she has developed jaundice.
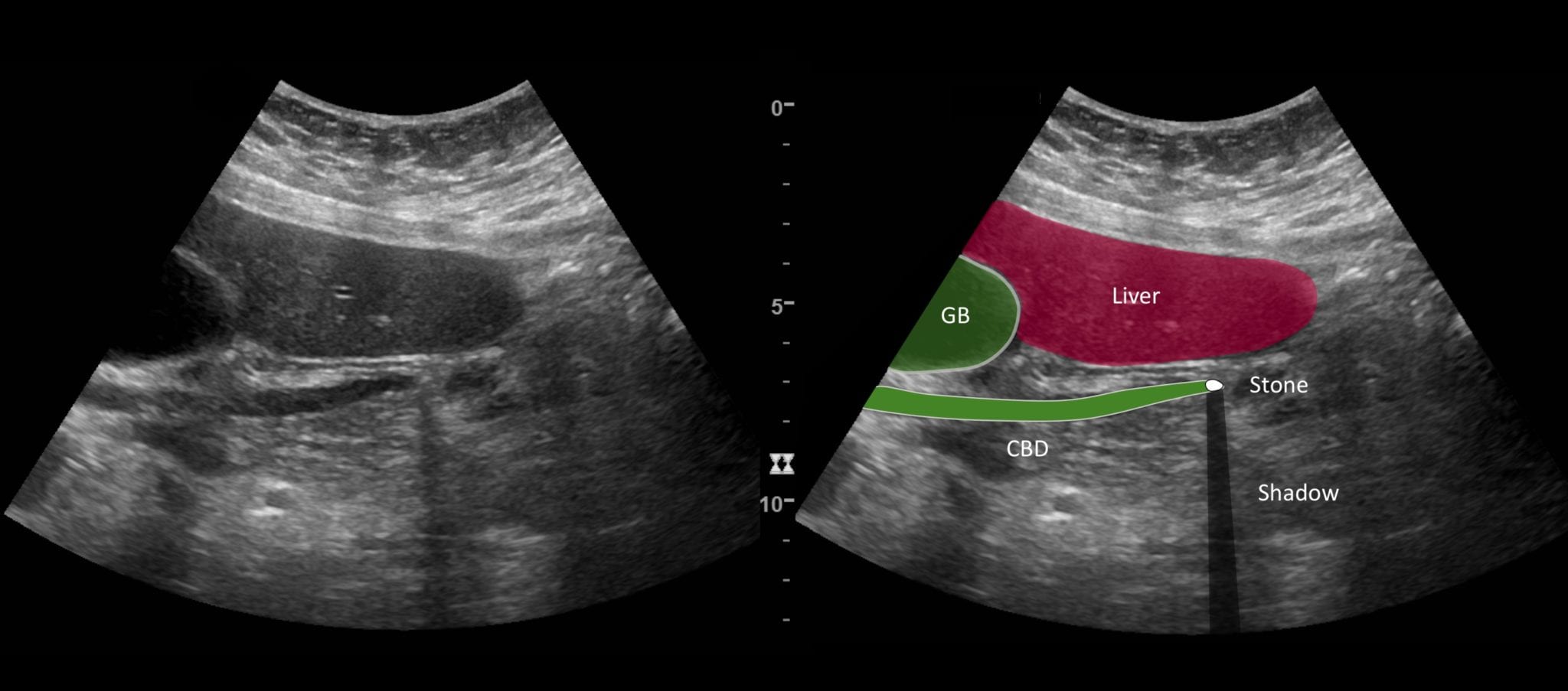
View 2: Longitudinal view of the distal common bile duct (CBD)
Describe and interpret these scans
IMAGE INTERPRETATION
Image 1: Longitudinal image of the gallbladder.
The gallbladder is distended, filled with sludge and several small gallstones. The wall is not thickened and there is no pericholecystic fluid.
Image 2: Longitudinal view of the distal common bile duct (CBD).
The duct is minimally dilated but a small echogenic, shadow casting calculus is seen in its distal end. An ERCP and stone retrieval is required. Cholecystectomy to prevent recurrence is also required.

CLINICAL CORRELATION
Choledocholithiasis.
Think about what you are looking for…before you scan. Then look really carefully for those things.
This was a case of painful obstructive jaundice. The intermittent nature of the pain made choledocholithiasis most likely. So I was primarily looking for a gallstone in the CBD – always keeping an open mind to other possibilities.
The small gallstones in the GB were easily seen, and further increased the probability of a small stone in the CBD. I measured the size of the CBD – at 8mm it was dilated. I looked for intrahepatic duct dilation – not much. Then followed the CBD to its distal end. The stone was subtle but definite, with the most obvious indicator of the actual stone the posterior acoustic shadowing.
Having confirmed choledocholithiasis the next question is about complications. There is pain and obstructive jaundice. But what about cholangitis and cholecystitis? The GB was dilated and clearly there was stasis with layering sludge, but the wall was not thickened, nor particularly tender, not hyperaemic and there was no pericholecystic fluid. Signs of cholangitis are subtle but the periportal echogenicity was absent and clinically fever was absent and inflammatory markers only slightly elevated.
Finding the CBD is challenging. Understanding its relationship to the head of the pancreas and the portal vein helps immensely.
When actually looking for the CBD I begin with a transverse view of the pancreas in the epigastrium. A cross sectional image of the distal CBD is attained. I then rotate the transducer 90 degrees clockwise and try to get a longitudinal view of the distal CBD. Next with the transducer rotated to about 10 o’clock I try to find the mid CBD from the subcostal view, angling up under the ribs. The next step is to approach from the anterior axillary line with the transducer lying in the intercostal space. Find the portal vein and angle slightly anteriorly to find the CBD in long section. I then repeat this with the patient lying in the left lateral decubitus position. This moves bowel and associated gas that may have been obscuring the view previously, and shifts the liver medially and inferiorly slightly which can help gain a better acoustic window. Asking the patient to take deep breaths can also help in finding the best window possible.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |