
![]()
Ultrasound Case 081
Presentation
A 70 year old man was admitted to hospital with a “viral illness”. A peripheral IV cannula was inserted into his right cubital fossa. It was never used and reportedly not checked until his wife, a nurse, complained saying it was red and hot and needed removal. The patient was discharged but a day later presents to your ED feeling generally unwell.
You take a look at the arm…

Image 2: Transverse cubital fossa to axilla
Image 3: Axillary to brachial vein: longitudinal
Image 4: Compression of the axillary vein
Describe and interpret these scans
IMAGE INTERPRETATION
Image 1: The upper arm is red, hot and swollen over the medial aspect from PIVC insertion site at the cubital fossa, to the upper arm.
Image 2: Cubital fossa to axilla:Transverse
In transverse you follow the medial cubital vein, to basilic vein to axillary vein. There is occlusive thrombus within the medial cubital vein and basilic vein. Fresher more hypoechoic clot extends into the axillary vein where is is non-occlusive and waves like a frond of seaweed, washed by the flow of surrounding blood. The occlusive thrombus distends the basilic vein wall. The surrounding subcutaneous fat is echogenic and oedematous, indicative of inflammation.
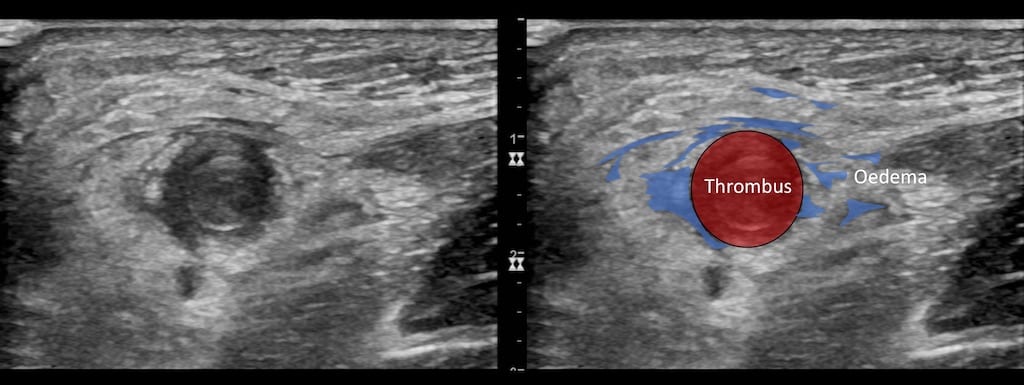
Image 3: Longitudinal view of the axillary vein, proceeding distally along the basilic vein.
Thrombus has formed initially in the non-distended basilic vein. In response the vein has distended, allowing flow past the obstruction, but then further thrombus has formed filling the entire lumen and keeping the vein distended. It creates a lamellated appearance.
Image 4: Compression of the axillary vein
Transverse view of the axillary vein with probe compression. There is partial compression with the thrombus preventing coaptation of the opposing vessel walls.
CLINICAL CORRELATION
Thrombophlebitis and upper limb DVT
Peripheral intravenous catheters are frequently associated with thrombophlebitis. This venous irritation and inflammation may be chemical, mechanical or infectious.
In this case nothing was administered intravenously and so chemical phlebitis is unlikely.
The cannula was sited at the right cubital fossa in a right handed man. With constant elbow flexion and extension mechanical irritation of the vein is common.
The most feared complication is infectious phlebitis and in this case where the patient felt systemically unwell, had raised inflammatory markers, and the erythema and inflammatory changes extended well beyond the bounds or the vessel infection was suspected.
In addition the thrombus had extended into the deep venous system. He was managed with antibiotics and anticoagulation – and followed up carefully to ensure resolution!
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |