![]()
Ultrasound Case 084
Presentation
A 23 year old man presents with presumed Achilles rupture. It’s an odd age to rupture one’s Achilles tendon and he hasn’t been on fluoroquinolones so you take a look. He described a few weeks of heel pain – Achilles tendon enthesopathy type pain.
A skateboard then entered the picture (as is so often the case). Whilst pushing on the ground to propel himself forward he felt sudden pain and a snap in his heel. He initially thought he has just hit a rock on the skateboard but soon realised he couldn’t walk and his heel pain was severe. There was bruising around his heel, a gap in the normal Achilles tendon just above the calcaneum, and a fullness above this.
So you wonder about an Achilles avulsion rather than rupture and put on the ultrasound transducer.

View 2
View 3
Describe and interpret these scans
IMAGE INTERPRETATION
Image 1: Panoramic view of the Achilles tendon in longitudinal.
The calcaneus is seen on the right. Immediately above this is a gap filled with blood. Further cranially the distal end of the Achilles is seen, with a calcified focus (echogenic with dense posterior acoustic shadowing) – representing the avulsed bony fragment from the calcaneus. Above this the Achilles tendon itself is seen. Folds within the retracted tendon are evident. These aren’t tears, but simply folds in the Achilles which now has no distal anchor.

Image 2: Clip of the Achilles avulsion in longitudinal with gentle ankle dorsiflexion.
- The Achilles is absent, and the avulsed fragment and calcaneum move independently.
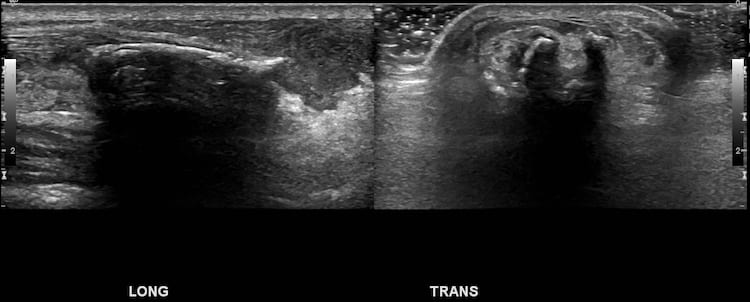
Image 3: A single longitudinal and transverse view of the avulsed fragment.
CLINICAL CORRELATION
Achilles tendon avulsion
This case demonstrates two things
The importance of a thorough clinical assessment and the utility of ultrasound in non-classic Achilles rupture cases – here the surgical approach will be significantly different to a standard Achilles rupture.
Anisotropy – the way a tendon appears as it curves in the ultrasound image. The tendon fibers reflect ultrasound back to the transducer beautifully when it runs perpendicularly to the ultrasound beam – and the fibers within the tendon are seen on the image. When the tendon curves and the fibers run obliquely or away from the ultrasound beam they seem to disappear and often cast a posterior acoustic shadow. This appearance is simply because ultrasound is not reflected directly back to the transducer by the linear fibers that are not perpendicular to the beam. In addition some edge shadow artefact may occur causing the deeper posterior acoustic shadowing.
The tip is not to call the hypoechoic area of tendon curving away within the field of view a tear – it is just a normal curve. This is commonly seen in the tendons of the rotator cuff, and a common pitfall for beginners.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |