
![]()
Ultrasound Case 099
Presentation
A 27 year old man presents with 10 hours of right testicular pain. He suffered minor trauma to the testis 20 hours prior to presentation and attributed the severe pain and swelling to that.
On examination the testis and epididymis were diffusely tender, firm and swollen, and seemed high riding and displaced medially. You consider torsion and trauma with haematoma most likely.
Image 2: Transverse scrotal scan centered on the right testis.
Image 3: Transverse view of the scrotum demonstrating both testes.
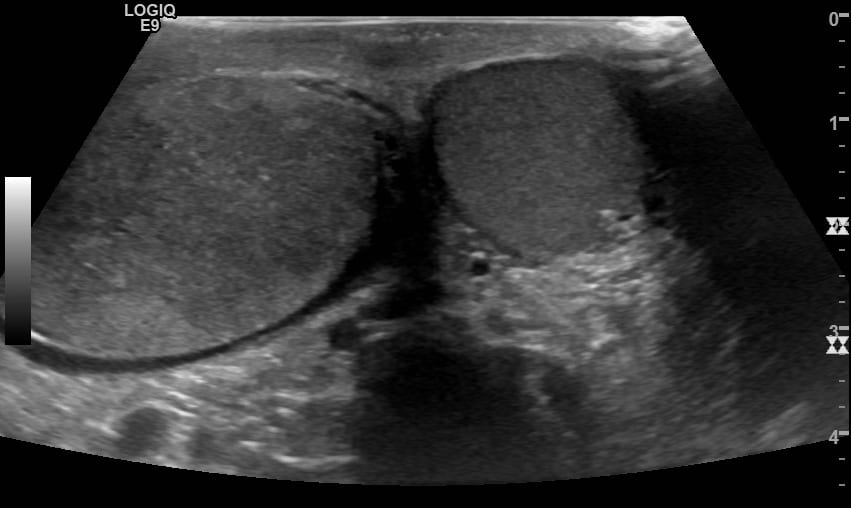
Image 4: Transverse view of the scrotum with Doppler

Image 5: Longitudinal views both testes with Doppler

Describe and interpret these scans
IMAGE INTERPRETATION
Image 1: Longitudinal scrotal scan across the right testis.
The testis is heterogeneous. The cord is oedematous and swollen and a cord knot is seen toward the end of the loop. A 720 degree torsion was evident at surgery.
Image 2: Transverse scrotal scan centered on the right testis.
Again the bulky right testis is markedly heterogeneous and the cord seen as bulky and knotted.
Image 3: Transverse view of the scrotum demonstrating both testes.
The right testis is enlarged and heterogeneous with a small hydrocele.
Image 4: Doppler is added and shows the right testis is completely ischaemic.
Image 5: Comparison of the right and left testis longitudinal views with Doppler interrogation.
The right testis is enlarged, hypoechoic and heterogeneous with a hydrocele and complete ischaemia.
CLINICAL CORRELATION
Testicular torsion with testicular ischaemia
Testicular torsion is a surgical emergency. In this case the testis had been completely ischaemic for 10 hours and was unsalvageable at surgery. Orchidectomy (removal) of the right testis was performed with orchidopexy (fixation to prevent future torsion) of the left testis.
Time is of the essence in cases of suspected testicular torsion. Traditionally a 4 hour maximal ischaemic time has been quoted for testicular survival, however it obviously depends on whether there has been complete, partial or intermittent testicular torsion.
In our institution when a case of acute scrotal pain with possible torsion presents we alert the urology team immediately and prepare the patient for theatre. As advanced emergency medical ultrasound is usually available immediately in our department, and does not delay the process, a scan is generally performed. We have found this useful in expediting transfer to theatre in true torsions, and in supporting clinical suspicion of other diagnoses when these occur.
The clinician should correlate the clinical and sonographic findings, always remembering that torsion detorsion, and partial torsion may not cause complete testicular ischaemia.Examine the cord and epididymis as well as the testis.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |