
![]()
Ultrasound Case 098
Presentation
A 55 year old man presents with upper calf tenderness and slight swelling. He has just returned from trekking in Nepal. He has a minor knee effusion clinically with tender subtle swelling of his upper calf. You consider the probable differential as DVT, calf muscle injury and Baker’s cyst with or without rupture.
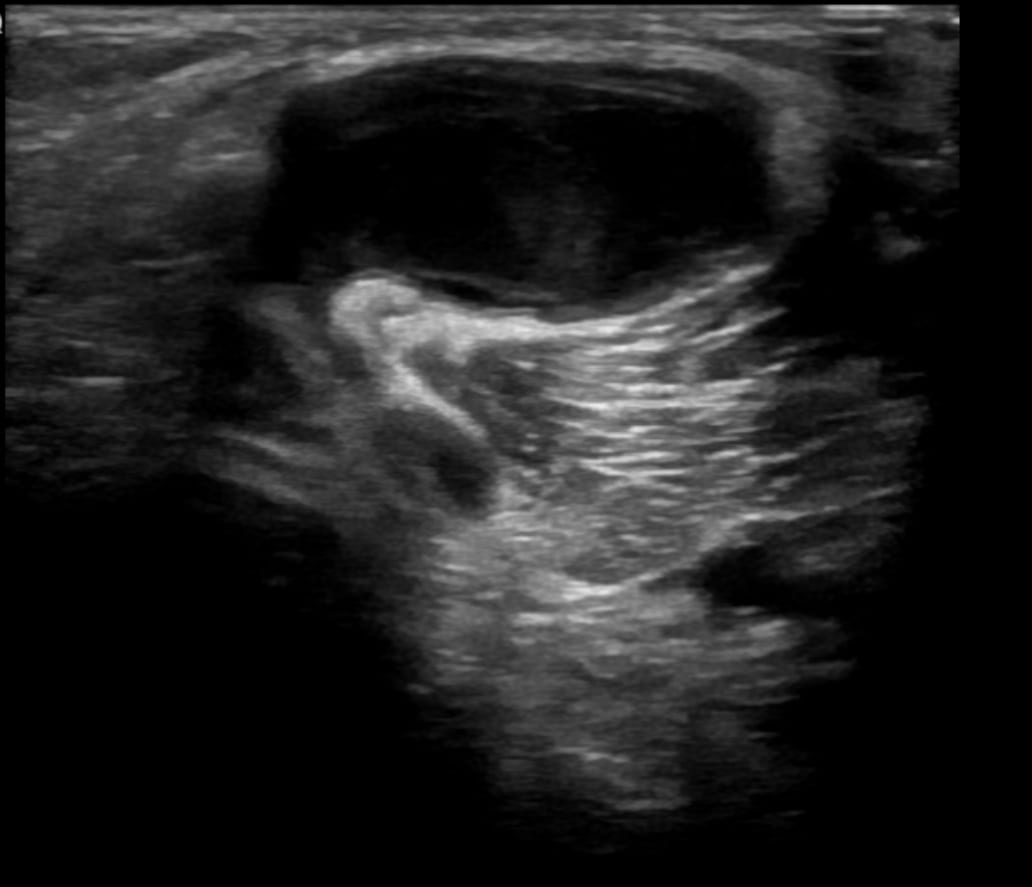
Image 2: Transverse view of the popliteal fossa.

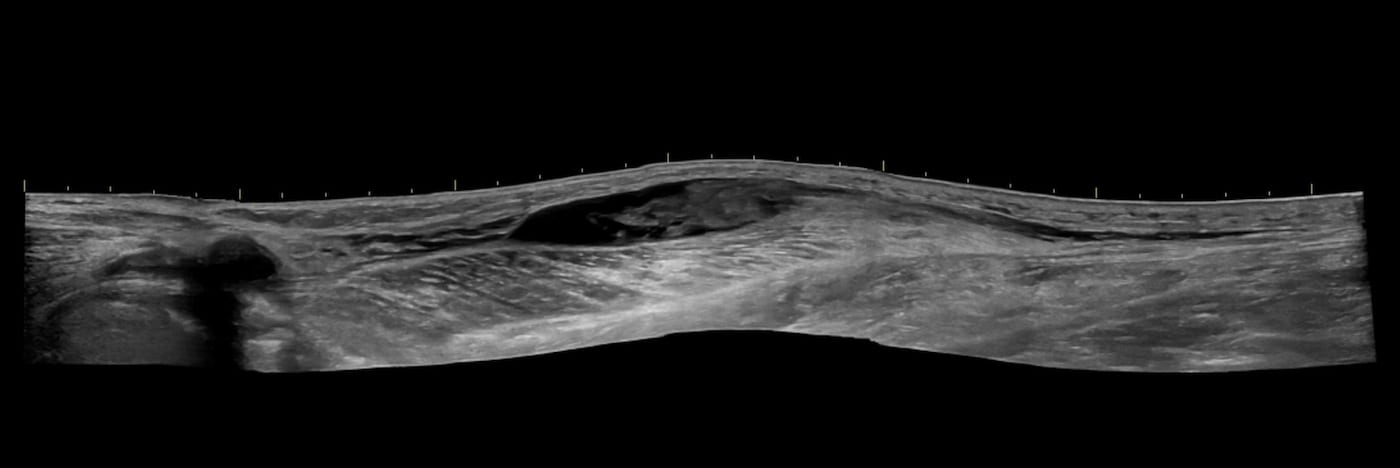
Image 3: Panoramic view, longitudinal section of the calf.
Describe and interpret these scans
IMAGE INTERPRETATION
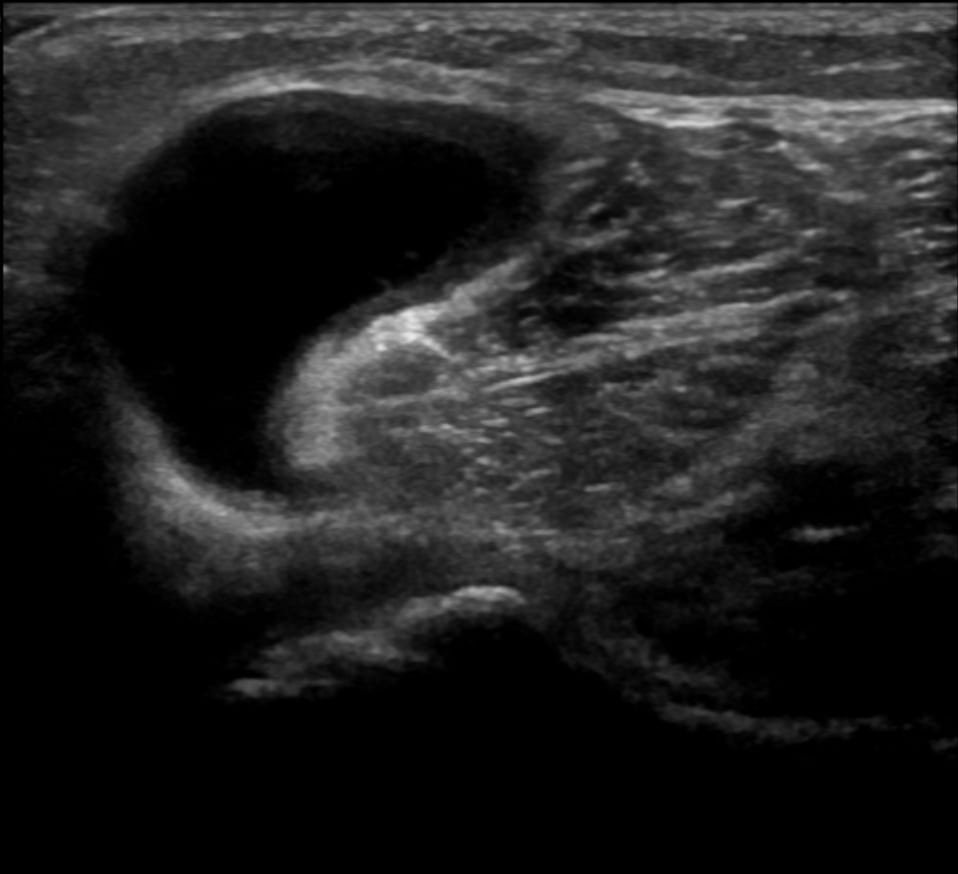
Image 1: Transverse view of popliteal fossa superior to inferior.
This demonstrates a Baker’s cyst (popliteal cyst)
Image 2: Transverse view of the popliteal fossa.
The Baker’s cyst has the classic “speech bubble” appearance.

Further examples of the classic “speech bubble” appearance of a Baker’s cyst.
The popliteal fossa.
In the adult population a Baker’s or popliteal cyst frequently occurs with an associated knee joint effusion. A communication between the medial posterior knee joint and the semimembranosus-gastrocnemius bursa occurs and fluid is pushed through a one-way valve like mechanism from the knee into the bursa. This bulges posteriorly and may cause pain and swelling, or rupture with fluid tracking inferiorly in the calf.
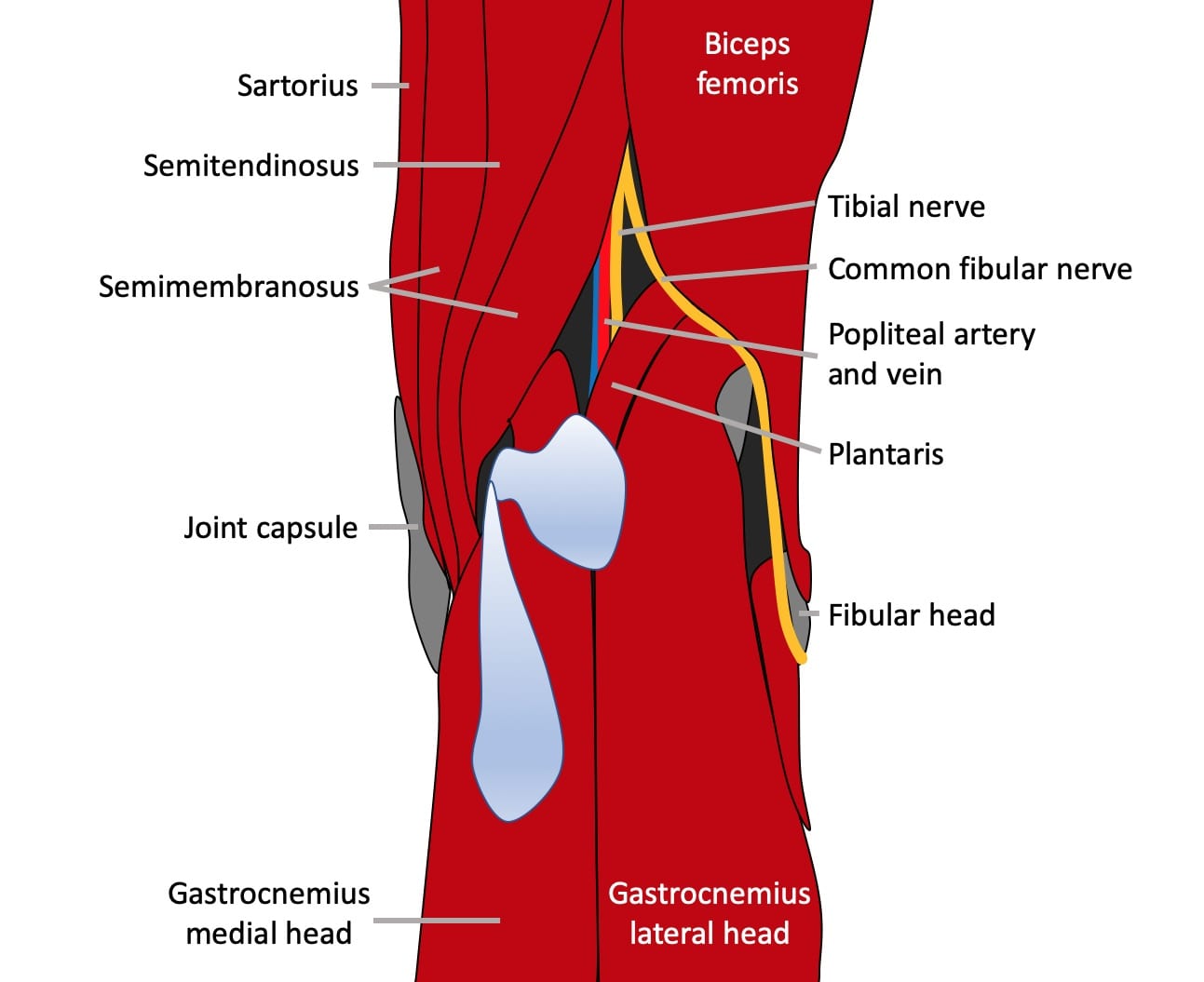
Image 3: Panoramic view, longitudinal section of the calf.
This shows a Bakers cyst which has ruptured. Fluid tracks into the superficial tissues of the calf, running along the surface of the gastrocnemius muscle. In this case there has been haemorrhage and clot is seen within the large calf collection. There is a relatively diverse appearance of complicated Baker’s cysts, with rupture, haemorrhage, internal debris and calcified loose bodies within the cyst as regular findings.
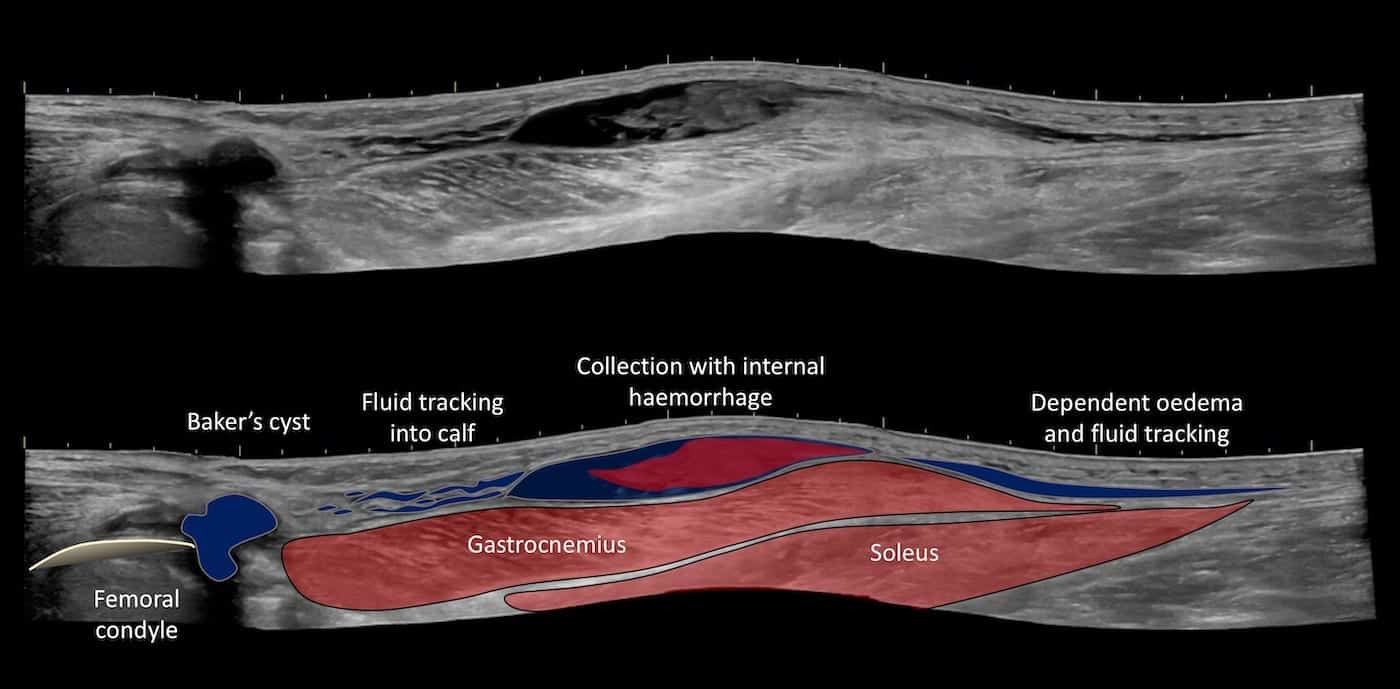
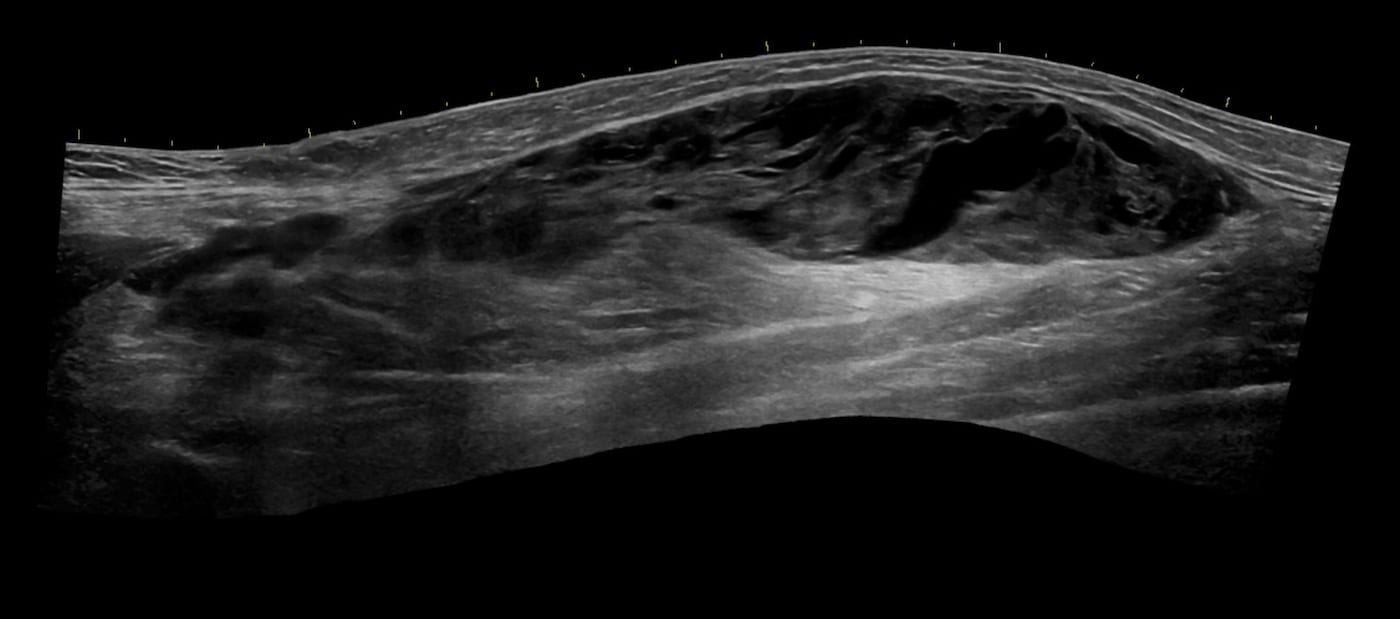
Image 4: Panoramic view longitudinal calf.
A large haemorrhagic collection in the superficial calf tissues secondary to a ruptured Baker’s cyst.
CLINICAL CORRELATION
A Baker’s or popliteal cyst is a frequent cause of posterior knee or calf pain.
It is important to consider alternate or concurrent diagnoses particularly deep vein thrombosis. The differential I have encountered as an Emergency Department sonologist is broad and has included:
- Baker’s or popliteal cyst.
- Deep and superficial vein thrombosis,
- Ischaemic lower leg due to peripheral vascular disease, thromboembolism or thrombosed popliteal aneurysm
- Traumatic muscle and tendon injuries such as calf muscle tear and / or haematoma (gastrocnemius, soleus or plantaris most commonly) and Achilles rupture
- Infective causes such as cellulitis or abscess formation
- Soft tissue tumours
- Referred radicular / neuropathic pain (sciatica).
FURTHER READING
- William Morrant Baker (1839 – 1896)
- Baker WM. On the formation of synovial cysts in the leg in connection with disease of the knee-joint. Saint Bartholomew’s Hospital Reports, London, 1877; 13: 245-261
- Baker WM. The formation of abnormal synovial cysts in connection with the joints. II. Saint Bartholomew’s Hospital Reports, London, 1885; 21: 177-190.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |