
![]()
Ultrasound Case 104
Presentation
A 33 year old woman is hit in the left lower chest with a high speed hockey ball. She has moderate pain and some postural hypotension and tachycardia. FAST demonstrates a splenic laceration and rupture with free fluid, she has a CT and proceeds for embolisation.
Her initial FAST scan and her repeat LUQ view are shown here. A week later she represents with some shortness of breath. A repeat FAST scan is performed.

Views 2-4: Left Upper Quadrant (LUQ)

Views 5: Pelvis

Views 6-7: LUQ video 1 week post injury
Describe and interpret these scans
IMAGE INTERPRETATION
Image 1: RUQ view initial scan.
A small amount of free fluid is seen in Morison’s pouch.
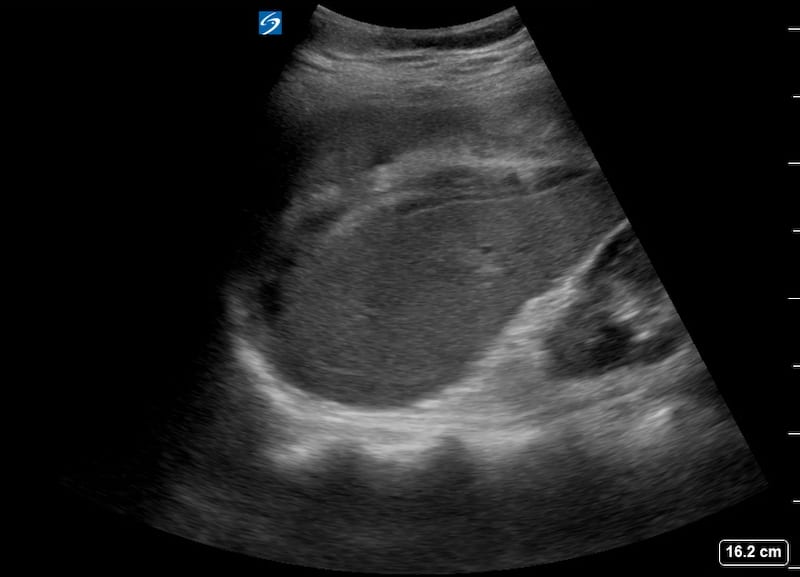
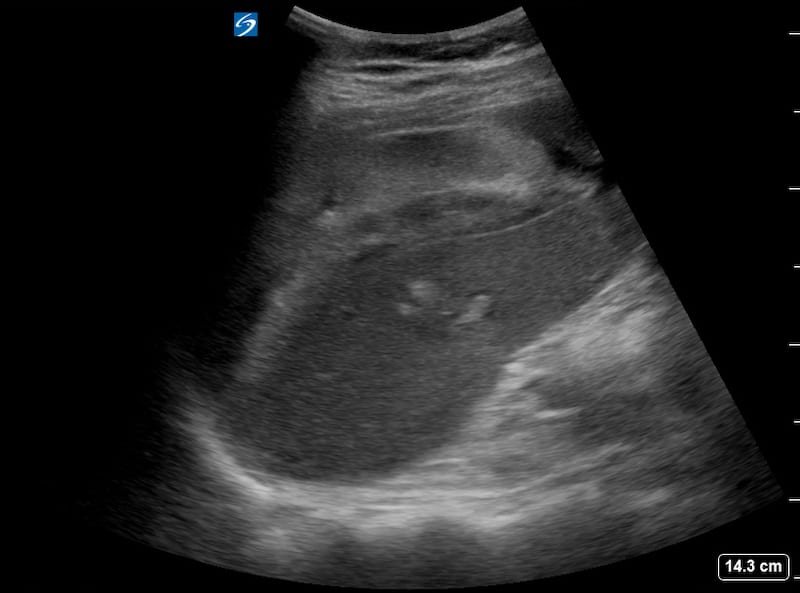
Image 2-4: LUQ views.
There is heterogeneous predominantly hyperechoic perisplenic haematoma as well as subcapsular haematoma. The echogenic area in the mid portion of the spleen disturbing the usual homogeneous echotexture suggests a laceration.
Image 5: Pelvis.
There is free fluid in the plevis lying adjacent to the bladder which is contained within the rounded bladder wall. In the clinical context this is blood.
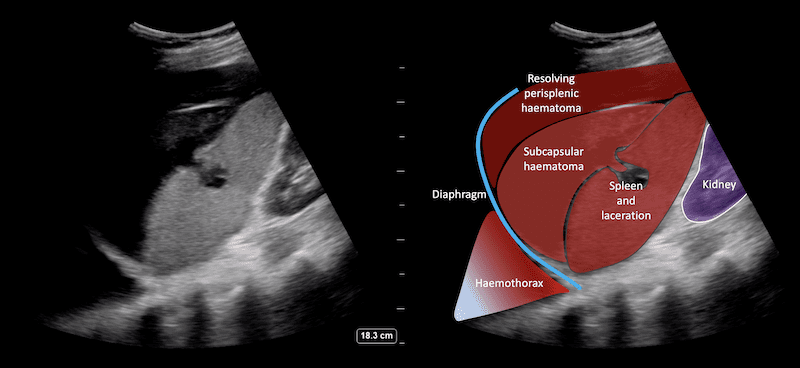
Image 6 and 7: LUQ video 1 week post injury.
The organising / resolving subcapular and perisplenic haematomas are far more hypoechoic. The defect in the spleen is more clearly deomonstrated and the echogenic coils clearly seen lying with in the spleen. In addition there is now a pleural effusion / haemothorax demonstrated above the diaphragm which is probably the cause of her new symptoms.
FURTHER IMAGING
Image 9-10: CT scans initial and 1 week following injury for correlation.
CLINICAL CORRELATION
Traumatic splenic rupture with subcapsular and perisplenic haematoma and haemothorax.
This is a fairly straight forward positive FAST scan. The combination of clearly directed LUQ mechanism of injury and abnormality on ultrasound including interruption of the normally homogeneous splenic echotexture and perisplenic haematoma make the diagnosis clear. It is a nice example of how the echogenicity of haematoma over time changes.
Acute clot is quite echogenic and can be difficult to differentiate from normal splenic, hepatic or retroperitoneal parenchyma. With time it becomes more hypoechoic and the splenic defect far more evident.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |