
![]()
W. Wayne Babcock

William Wayne Babcock Jr (1872-1963) was an American surgeon, educator, and surgical innovator
His name is attached to a diverse group of eponymous terms, including the Babcock operation for varicose veins, Babcock forceps, Babcock probe, Babcock sump drain, Babcock–Bacon operation, and the Babcock “soup bone” cranioplasty. He also contributed to nerve disassociation, alloy-steel wire sutures, early mesh hernia repair, aneurysm surgery, and surgical education through his Textbook of Surgery.
In anaesthesia, Babcock was one of the early American champions of spinal anaesthesia, regarding it as a highly technical method in which the surgeon’s injection determined the site, duration, and degree of block. His name is linked with the Quincke–Babcock spinal needle, a styleted cutting-bevel pattern associated with his spinal anaesthesia practice.
Biographical Timeline
- Born on June 10, 1872 in East Worcester, New York, USA to William Wayne Babcock (1842–1932) and Sarah Jane Butler (1843–1922)
- 1893 – Received his first medical degree from the College of Physicians and Surgeons, Baltimore.
- 1895 – Received a second medical degree from the University of Pennsylvania after postgraduate medical training.
- 1900 – Received a further doctorate from the Medico-Chirurgical College of Philadelphia.
- 1903 – Appointed Chair of Surgery and Clinical Surgery at Temple University, Philadelphia, at age 31. A post he held until 1943.
- 1907 – Introduced the Babcock operation for varicose veins, using an acorn-shaped probe to strip the saphenous vein. Associated with the introduction/popularisation of spinal anaesthesia in the United States.
- 1914 – Published the technic of spinal anesthesia describing his spinal anaesthesia technique and needle preferences.
- 1917–1919 – Served in the US Army Medical Corps during World War I, advancing to lieutenant colonel. Published his “Soup Bone” cranioplasty technique, using preserved bovine bone for cranial reconstruction.
- 1928 – Published a Textbook of Surgery for Students and Physicians a standard reference for generations of students and surgeons.
- 1928 – Published “Spinal anesthesia: an experience of twenty-four years”, describing his long experience with spinal anaesthesia, beginning after exposure to European practice in 1904.
- 1930–1945 – With Harry E. Bacon, developed and popularised the Babcock–Bacon operation, a sphincter-preserving pull-through procedure for cancer of the rectum and sigmoid colon.
- 1943 – Retired from the Chair of Surgery at Temple University after four decades of service.
- 1947 – Received the Master Surgeon Award from the International College of Physicians and Surgeons.
- 1954 – Awarded the American Medical Association Distinguished Service Medal for contributions including spinal anaesthesia, thyroid surgery, bone grafting, surgical instruments, and stainless-steel wire use in abdominal wounds.
- Died February 23, 1963, aged 90 at Bala-Cynwyd, Montgomery, Pennsylvania, USA
As we progress we lay aside the aids of previous days with grateful reverence, not with apology or disdain. We shall not scorn what was done yesterday because we have something better today any more than our interest in the past will cause us to continue the practice of the past.
Babcock WW, 1928
Key Medical Contributions
Spinal anaesthesia and the Quincke–Babcock needle
Babcock was an early American advocate of spinal anaesthesia and one of the surgeons credited with popularising its use in the United States. In 1914 he published The technic of spinal anesthesia reporting that he and fellow associates had performed spinal anaesthesia more than 6,000 times, using a range of intrathecal solutions including stovaine, tropacocaine, and novocaine. Babcock emphasised that successful spinal anaesthesia required careful patient selection, knowledge of drug spread, choice of interspace, and prompt operative technique.
His 1928 review Spinal anesthesia: An experience of twenty-four years, defined spinal anaesthesia as a highly technical method under the surgeon’s direct control. Babcock wrote that the operator’s injection determined the location, duration, and degree of anaesthesia, and warned that poor technique or inadequate supervision could be dangerous.
Quincke–Babcock spinal needle
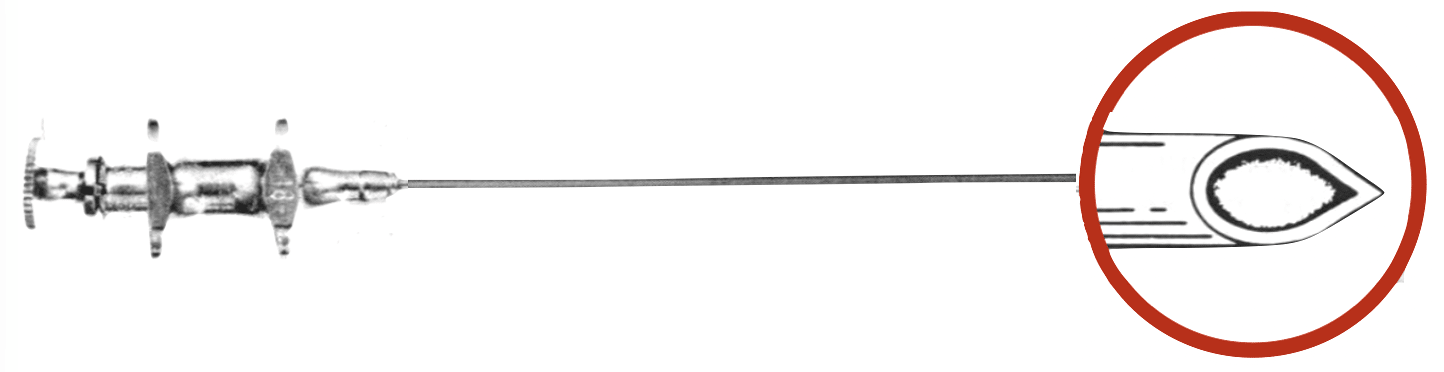
The Quincke–Babcock spinal needle is usually described as a smaller cutting-bevel spinal needle derived from the Quincke design. Typically 20G, with a medium bevel and matching stylet. The design preserved the reliable dural puncture and CSF return of a cutting needle, while reducing calibre and improving construction compared with earlier larger spinal needles.
Babcock’s 1914 apparatus description does not appear to use the eponymic term “Quincke–Babcock.” He described a 2 mL Luer-type syringe and a small, light spinal needle of iridium, platinum, or gold, approximately 7 cm long and 0.1 cm in diameter, fitted with a stylet to prevent obstruction during insertion.
Later commercial sources identify a Quincke–Babcock pattern spinal needle, such as the Becton Dickinson version described with a Luer-Lok hub, fitted stylet, and matched bevel point. The eponymous term applied to a styleted cutting-bevel spinal needle associated.
Babcock also refined a self-filling syringe for the introduction of spinal anaesthesic

Babcock operation for varicose veins
The Babcock operation was a vein-stripping procedure for varicose veins, introduced in Babcock’s 1907 paper new operation for the extirpation of varicose veins of the leg.
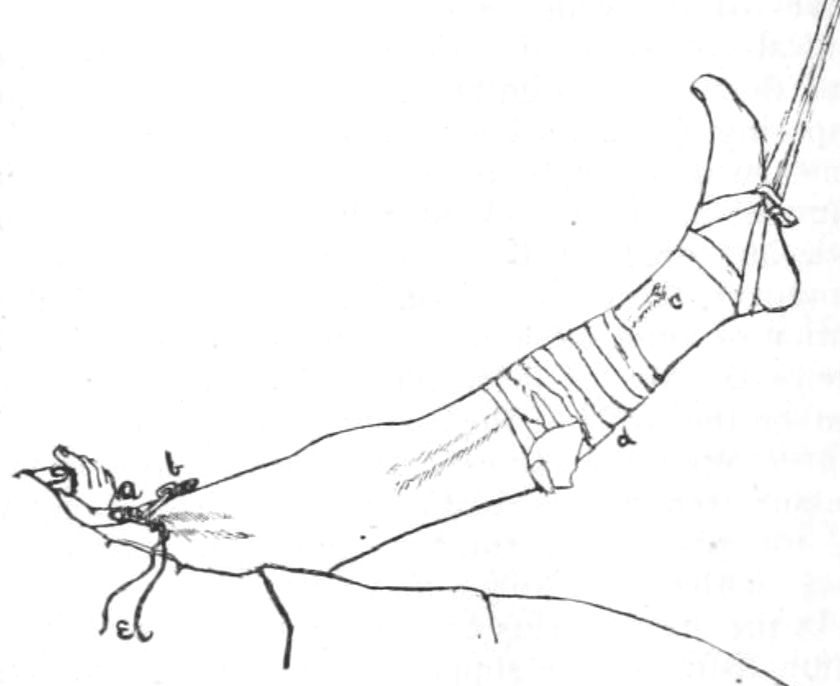
Babcock described removal of the long saphenous vein through small incisions using a flexible, double-ended extractor. The instrument had acorn-shaped bulbous tips and was passed within the vein; the vein was then tied to the shaft and withdrawn, stripping the vessel from surrounding tissues and tributaries. Babcock considered the method simpler, faster, and less traumatic than long open incisions or multiple segmental excisions.

The procedure became internationally associated with Babcock and his acorn-tipped vein stripper. It represented an early twentieth-century move toward less invasive venous surgery, replacing long open exposures with limited incisions and subcutaneous extraction of the diseased vein.
Babcock forceps and surgical instruments
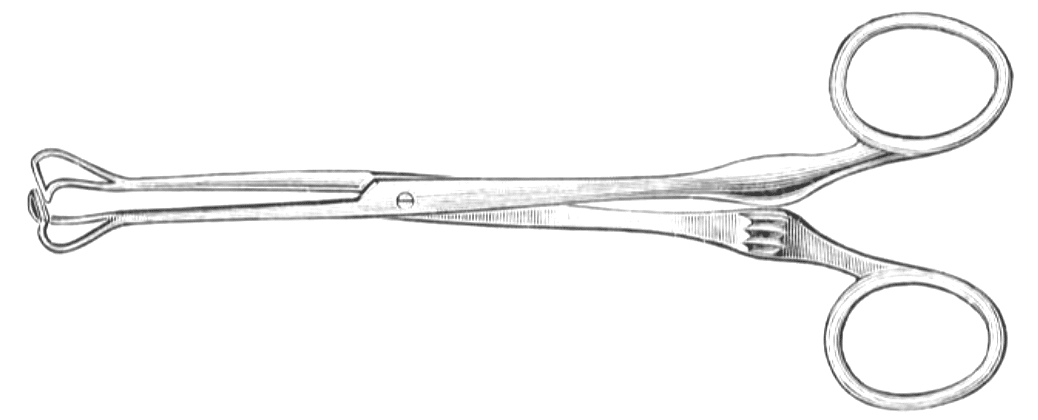
Babcock is associated with multiple surgical instruments, including the Babcock forceps, Babcock probe, and Babcock sump drain.
The Babcock forceps are non-traumatic tissue-holding forceps designed to grasp delicate structures without crushing them. Their fenestrated, rounded jaws distribute pressure and are commonly used to handle bowel, appendix, fallopian tube, and other tubular or fragile tissues. They remain one of Babcock’s most widely recognised surgical eponyms.
Babcock–Bacon operation for rectosigmoid cancer
The Babcock–Bacon operation was a sphincter-preserving pull-through procedure for carcinoma of the rectum and sigmoid colon. It developed from Babcock’s earlier work on eliminating permanent abdominal colostomy in selected patients with rectosigmoid cancer.
In his 1932 paper, The operative treatment of carcinoma of the rectosigmoid with methods for the elimination of colostomy Babcock described modifications to conventional abdominoperineal resection. His aimed to avoid routine abdominal colostomy, reduce pelvic contamination, close the pelvic cavity rapidly, deliver the diseased bowel through the perineum without rupture, and form a satisfactory perineal colostomy.
Babcock’s method used a “safe pull-through” principle. The diseased bowel was not dragged through the pelvis by traction on friable malignant tissue. Instead, a soft gauze band was tied around the sigmoid well above the carcinoma, packed against the pelvic floor, and later used to deliver the liberated bowel through the perineal incision. His paper illustrated several older pull-through methods and warned that traction through malignant tissue risked rupture and contamination.
1952 – The later Babcock–Bacon operation, with Harry E. Bacon at Temple University, extended this sphincter-preserving philosophy. It was an influential but controversial operation for rectal and rectosigmoid cancer, particularly where preservation of continence and avoidance of permanent abdominal colostomy were major goals.
“Soup bone” cranioplasty
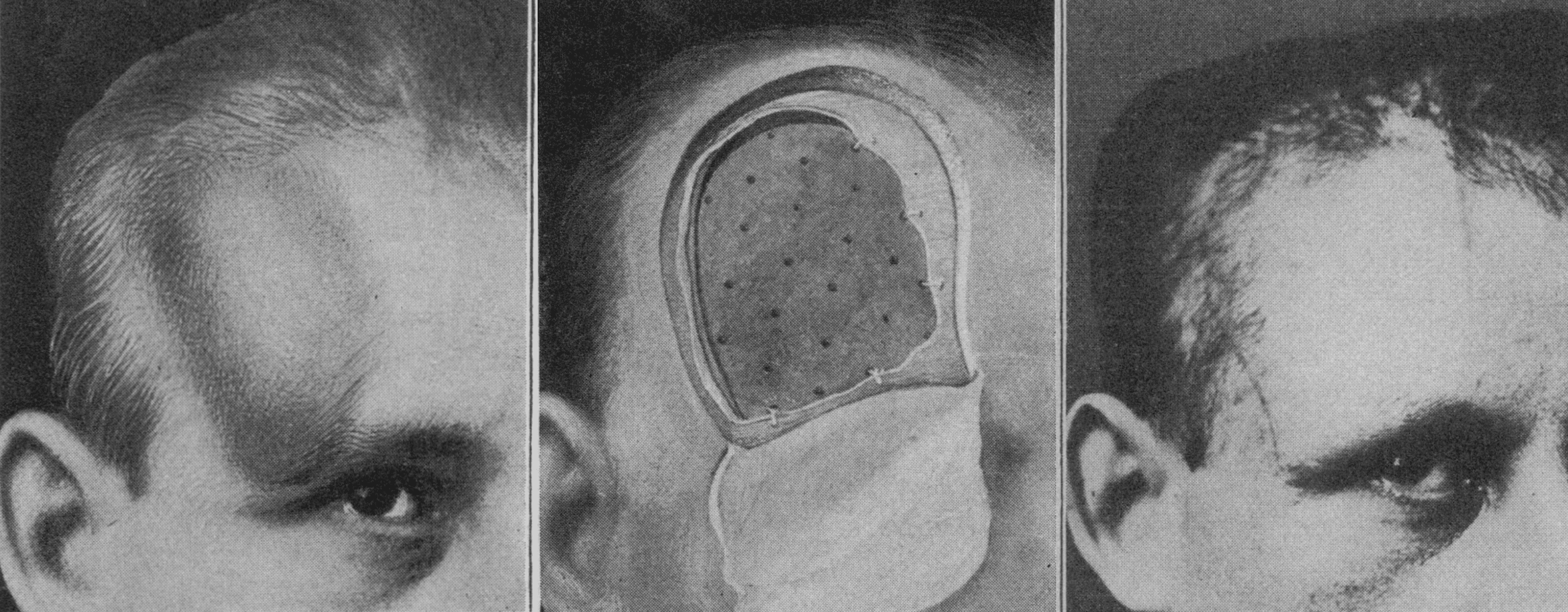
Babcock’s “soup bone” cranioplasty was an inventive early reconstructive technique for skull and facial defects. In his 1917 JAMA paper, Babcock reported five cases in which portions of beef or mutton bone from the hospital “soup-kettle” were implanted beneath the scalp or facial skin to restore contour and support.
He proposed the method at a time when surgeons were experimenting with metal, ivory, celluloid, paraffin, cork, autogenous bone, and other materials for cranial reconstruction. Babcock preferred prepared animal scapula because it was accessible, thin, porous, and large enough to shape. The bone was reboiled, soaked in phenol, boiled again, trimmed, drilled, and fitted into or over the defect beneath the periosteum or scalp.
The ‘soup bone’ implant here advocated has not only the advantages of convenient accessibility, mobility and sufficient size, but apparently produces, when embedded, little or no irritation of the adjacent tissue, and seems to give a strong and perhaps permanent closure.
Babcock 1917
Babcock did not claim that the dead animal bone simply remained unchanged. Rather, he suggested that it might act as a scaffold for ingrowth of firm tissue or new vascularised material:
It is probable that the dead bone serves as a scaffold for the ingrowth of new firm tissue
In later discussion he was appropriately cautious, noting that the long-term fate of such implants remained uncertain, but that retained skull implants after two years made the method “worth trying.” The technique did not become a durable standard reconstructive method, but it remains a memorable example of pragmatic early twentieth-century surgical innovation.
Nerve dissociation / nerve disassociation
Babcock used his nerve disassociation technique for painful or paralytic disorders of nerve trunks caused by injury, inflammation, neuritis, or cicatricial compression. In his 1907 preliminary report, he described treating affected nerves by exposing the nerve through an incision, opening the nerve sheath longitudinally, carefully separating the component nerve fibres, and isolating the nerve from surrounding scar or fibrous tissue.
Babcock intended the operation to decompress the nerve, release intraneural exudate, free nerve fibres trapped in scar tissue, and encourage restoration or formation of nerve pathways. He considered it a more conservative alternative to nerve stretching, resection, or bridging with foreign material in selected cases.
In four reported operative cases, Babcock described relief of pain in three and immediate reduction of palsy in three. He concluded that nerve disassociation was “less dangerous and more potent” than nerve stretching in certain cases of neuritis, and might be worth trial in peripheral paralysis due to interruption of nerve pathways by fibrous tissue.
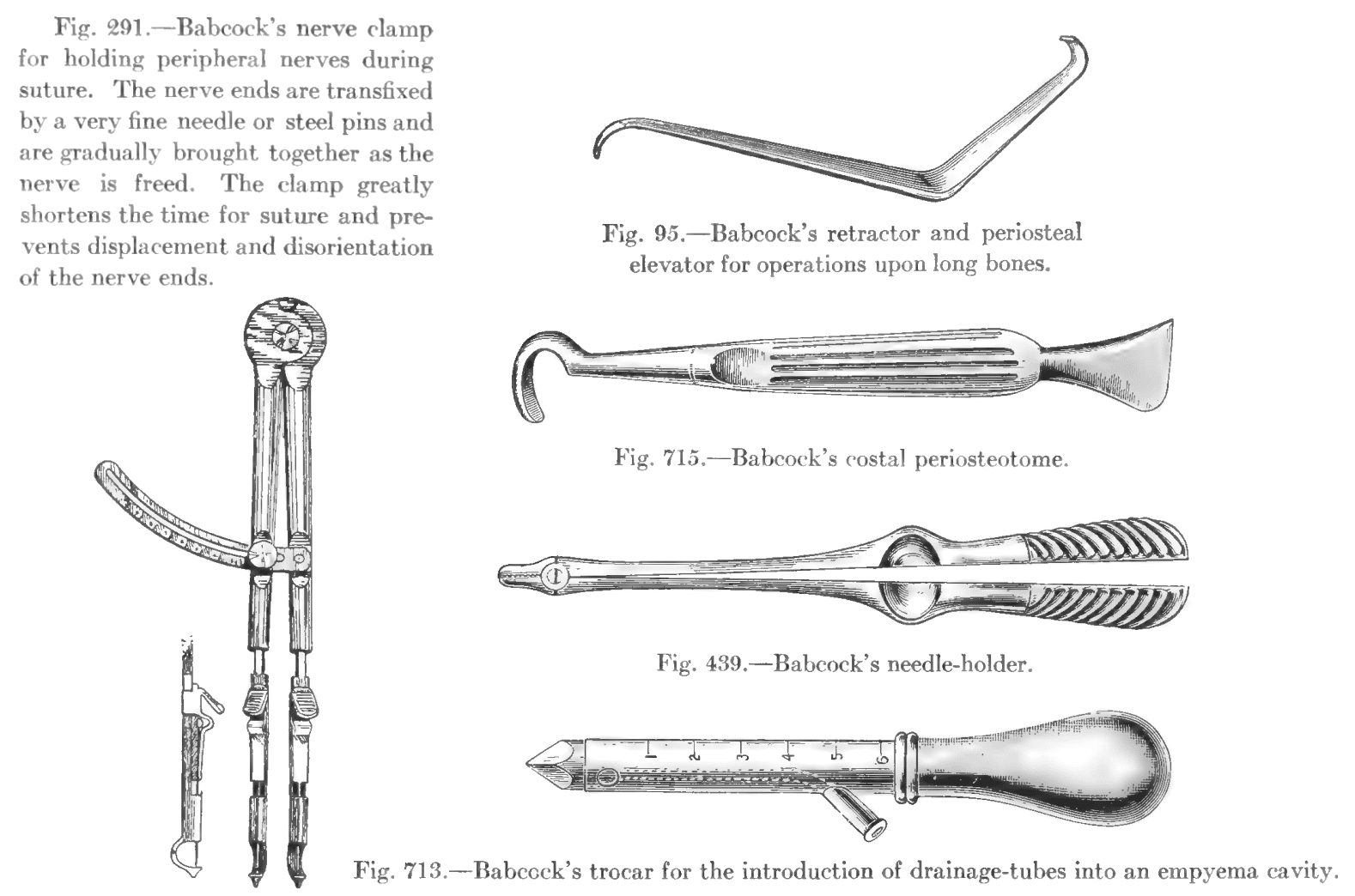
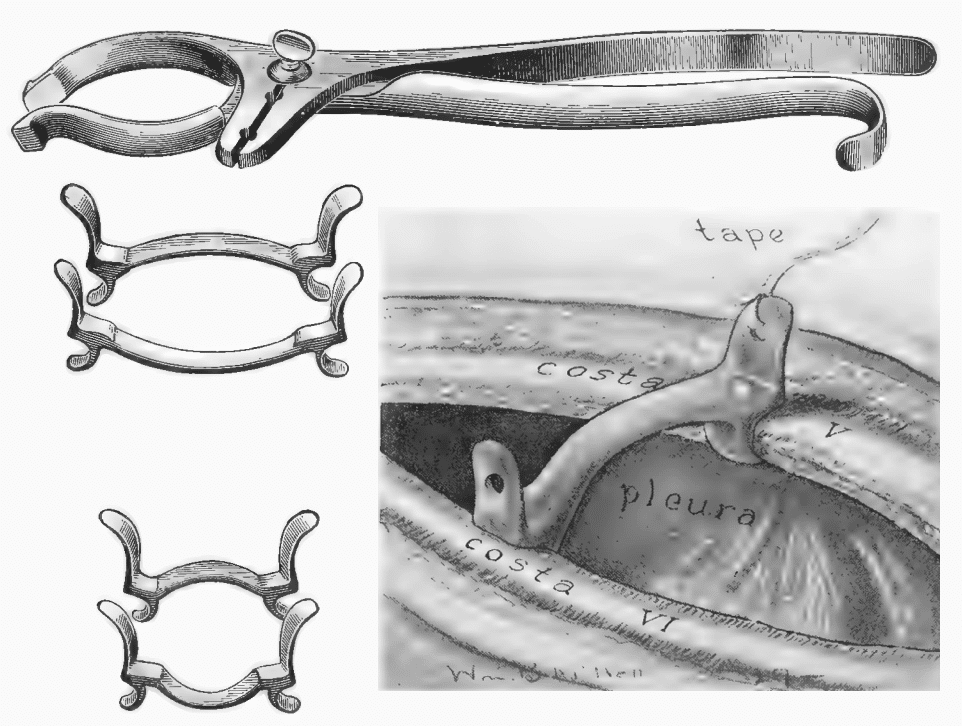
Babcock Instruments
Major Publications
- Babcock WW. Nerve Disassociation; A New Method for the Surgical Relief of Certain Painful or Paralytic Affections of Nerve Trunks. Ann Surg. 1907 Nov;46(5):686-93.
- Babcock WW. A new operation for the extirpation of varicose veins of the leg. New York medical journal 1907; 86: 153.
- Babcock WW. Spinal anesthesia : a study of 658 administrations. 1909
- Babcock WW. The technic of spinal anesthesia. New York Medical Journal. 1914; 100(15): 697–702
- Babcock WW. “Soup Bone” implant for the correction of defects of the skull and face JAMA 1917; LXIX(5): 352-355.
- Babcock WW. Spinal anesthesia in relation to associated therapeutic problems. May 16, 1923 New York medical journal and Medical Record
- Babcock WW. A new treatment of thoracic aneurysm. Annals of Clinical Medicine, 1926; 4: 933-942 [Babcock’s operation for thoracic aneurysm]
- Babcock WW. Spinal anesthesia: An experience of twenty-four years The American Journal of Surgery 1928; 5(6): 571-576
- Babcock WW. A Textbook of surgery. Philadelphia, Saunders, 1928 [2e 1935]
- Babcock WW. Operative decompression of aortic aneurysm by carotid-jugular anastomosis. Surgical Clinics of North America, Philadelphia, 1929; 9(5): 1031-1041. [Babcock’s operation for aortic aneurysm]
- Babcock WW. The operative treatment of carcinoma of the rectosigmoid with methods for the elimination of colostomy. Surgery, Gynecology and Obstetrics. 1932; 55: 627–632.
- Babcock WW. Ligatures and sutures of alloy steel wire. JAMA 1934;102;(21):1756
- Babcock WW, Bacon HE. Operative treatment of cancer of the large bowel without colostomy. Arch Surg 1943;46;(2):253-264.
- Babcock WW, Bacon HE. An Evaluation of Operations Used for Carcinoma of the Large Bowel. Western Journal of Surgery, Obstetrics, and Gynecology 1952; 60(4): 141
- Bacon HE. Cancer of the Colon, Rectum and Anal Canal: surgical approach with rates of five and ten year survival. The American Journal of Surgery 1957; 94(4): 567-572
References
Biography
- Dr. William W. Babcock awarded distinguished service medal. JAMA 1954;155;(10):912
- Rosenberg H, Axelrod JK. Two surgeons who popularized spinal anesthesia. Reg Anesth Pain Med. 2001 May-Jun;26(3):278-82
Eponymous terms
- Corman ML. William Wayne Babcock 1872-1963. The Operative treatment of carcinoma of the rectosigmoid with methods for the elimination of colostomy. Dis Colon Rectum. 1989 May;32(5):442-7
- Haubrich W. Babcock of the Babcock Clamp. Gastroenterology 2001; 121(2): 244
- Sandler AL, Biswas A, Goodrich JT. The Reverend Russell H. Conwell, W. Wayne Babcock, and the “soup bone” cranioplasties of 1915. Neurosurg Focus. 2014 Apr;36(4):E21.
- Laios K. Professor William Wayne Babcock (1872-1963) and His Innovations in Surgery. Surg Innov. 2018 Oct;25(5):536-537.
- Harms R, Cadogan M. History of Spinal Needles. LITFL
Eponym
the person behind the name

MBBS, Curtin University. Junior doctor working at Sir Charles Gairdner Hospital. Interested in Emergency Medicine, education and baking.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
