
![]()
Wallenberg Syndrome
Description
Wallenberg Syndrome (aka: lateral medullary syndrome or the posterior inferior cerebellar artery syndrome) is a neurological disorder with a variety of symptoms associated with posterior circulation ischaemic stroke.
The infarcted area in Wallenberg syndrome is supplied by the posterior inferior cerebellar artery (PICA) usually secondary to atherothrombosis of the vertebral artery (80%), or posterior inferior cerebellar artery.
High-risk group is typically the elderly vasculopath presenting with dizziness/vertigo, loss of balance with gait instability, hoarse voice and difficulty swallowing.
| General Symptoms | Ipsilateral Signs | Contralateral Signs |
| Vertigo | Horner syndrome (ptosis, miosis, hypohidrosis or anhidrosis, enophthalmos, due to damage to descending sympathetic fibers) | Spinothalamic loss (loss of pain/temperature) in trunk and limbs |
| Diplopia | Cerebellar signs ataxia / nystagmus with a tendency to fall towards the side of the lesion; nystagmus can have both horizontal and rotational components | Hyperhidrosis |
| Dysphagia | IX and X cranial nerve palsy Loss of taste, to posterior one third of tongue; palatal paralysis); reduced gag reflex; dysphagia; dysphonia (paralysis of the ipsilateral vocal cord). | |
| Autonomic disturbance (Tachycardia/bradycardia/ labile blood pressures) [Thought to be due to involvement of the dorsal motor nucleus of the vagus nerve] | Spinothalamic sensory loss in the face (in the medulla the trigeminal spinothalamics have not yet crossed) Neuralgic pain can also be experienced, (essentially a rare form of trigeminal neuralgia) |
History of the Wallenberg Syndrome
1807 – On December 29, Geneva physician Gaspard Vieusseux (1746-1814) suffered a sudden illness that he later described before the Société médico-chirurgicale de Genève in 1808.
Original
English
Engourdissement du côté gauche de la face, avec perte remarquable de sensibilité pour la chaleur et le froid, quoique le tact restât intact; affection semblable du bras et de la jambe du côté droit; difficulté considérable d’articulation, constriction du pharynx avec gêne à la déglutition; enrouement de la voix; langue déviée à gauche; hoquet presque continuel; chute de la paupière supérieure gauche
Numbness of the left side of the face, with remarkable loss of sensitivity to heat and cold, although touch remained intact; similar affection of the arm and leg on the right side; considerable difficulty in articulation, constriction of the pharynx with difficulty in swallowing; hoarseness of voice; tongue deviated to the left; almost continual hiccups; drooping of the left upper eyelid
Vieusseux 1808 (Odier recount 1915)
1810 – Alexander Marcet (1770-1822) reproduced Vieusseux’s case for the Royal Society and published the account in Medico-Chirurgical Transactions (1811)
On the 29th of December, 1807, Mr. Vieusseux was suddenly seized with a numbness of the left side of the face, attended with a remarkable loss of sensibility to heat and cold, while the sense of touch remained unimpaired. Soon afterwards, a similar affection attacked the right arm and leg. The patient experienced at the same time considerable difficulty in articulation, a sense of constriction in the pharynx impeding deglutition, and a hoarseness of the voice. His tongue deviated to the left side when protruded; he was tormented by almost continual hiccup, and the upper eyelid of the left eye appeared to fall down from diminished power of the levator muscle
Marcet, 1811
Following the death of Vieusseux in 1814, Marcet writes ‘it is much to be regretted that his head was not opened.‘
1811 – Hermann Senator (1834-1911) described a case of a 56-year old ex-baker exhibiting the clinical features seen in lateral medullary syndrome, however could not identify the origin of the lesion.
1894 – Adolf Wallenberg intricately detailed the clinical findings of a 38-year old man with the syndromic features. His findings, alongside a detailed examination of seven brains, and the anatomical work of Henri Duret (1849-1921), allowed him to accurately localise the site of the lesion.
German
English
Zwei bis drei Monate nach dem Insult etwa folgender Status:
Subjective Symptome:
1. Schwindel, Neigung nach links zu fallen.
2. Taubheitsgefühl in der linken Gesichtshälfte, rechten Körperhälfte mit Ausnahme des Gesichtes.
3. Schluckbeschwerden (sehr gering).
4. Schmerzen im Nacken, zuweilen auch im linken Auge.
Objective Symptome:
1. Schwanken nach links beim Gehen.
2. Ataxie der linken Extremitäten (nur noch angedeutet).
3. Parese der linken Gaumensegelhälfte.
4. Paralyse, später Parese des linken Stimmbandes (Andeutung von Atrophie?).
5. Grösseres Volumen der linken Zungenhälfte bei ruhiger Lage im Munde.
6. Sensibilitätsstörung im Bereiche des ersten, weniger des zweiten Astes des linken Trigeminus, namentlich Auge, Lider, Nasenrücken und Nasenschleimhaut betreffend…
7. Fehlen des linken Comeal- und Conjunctivalreflexes.
8. Störungen des Schmerzund Kältegefühls an der rechten Rumpfhälfte…
9. Alterationen der übrigen Empfindungsqualitäten (namentlich Ortssinn, faradocutane Sensibilität, Drucksinn) in geringem Grade…
10. Andeutimg von Ataxie des linken Beines ohne Störung der groben Kraft.
11. Fehlen der Bauchreflexe.
In den folgenden Wochen verschwinden allmälig die Schluckbe- schwerden, die Neigung nach links zu fallen, die Ataxie; die anderen Erscheinungen, namentlich die Stimmband-, Zungen-, Gaumenparese und die SensibilitätsstOrungen bleiben im Wesentlichen stationär. Dazu gesellt sich ein neues Symptom:
12. Bei der Auscultation des rechten Warzenfortsaties systolisches Geräusch, das sich nach hinten bis zur Grista occipitalis, nach unten bis zum Unterkieferwinkel, nach vorne (sehr schwach!) bis zur Schläfe verfolgen lässt. Pulsation der Halsgefässe rechts stärker als links.
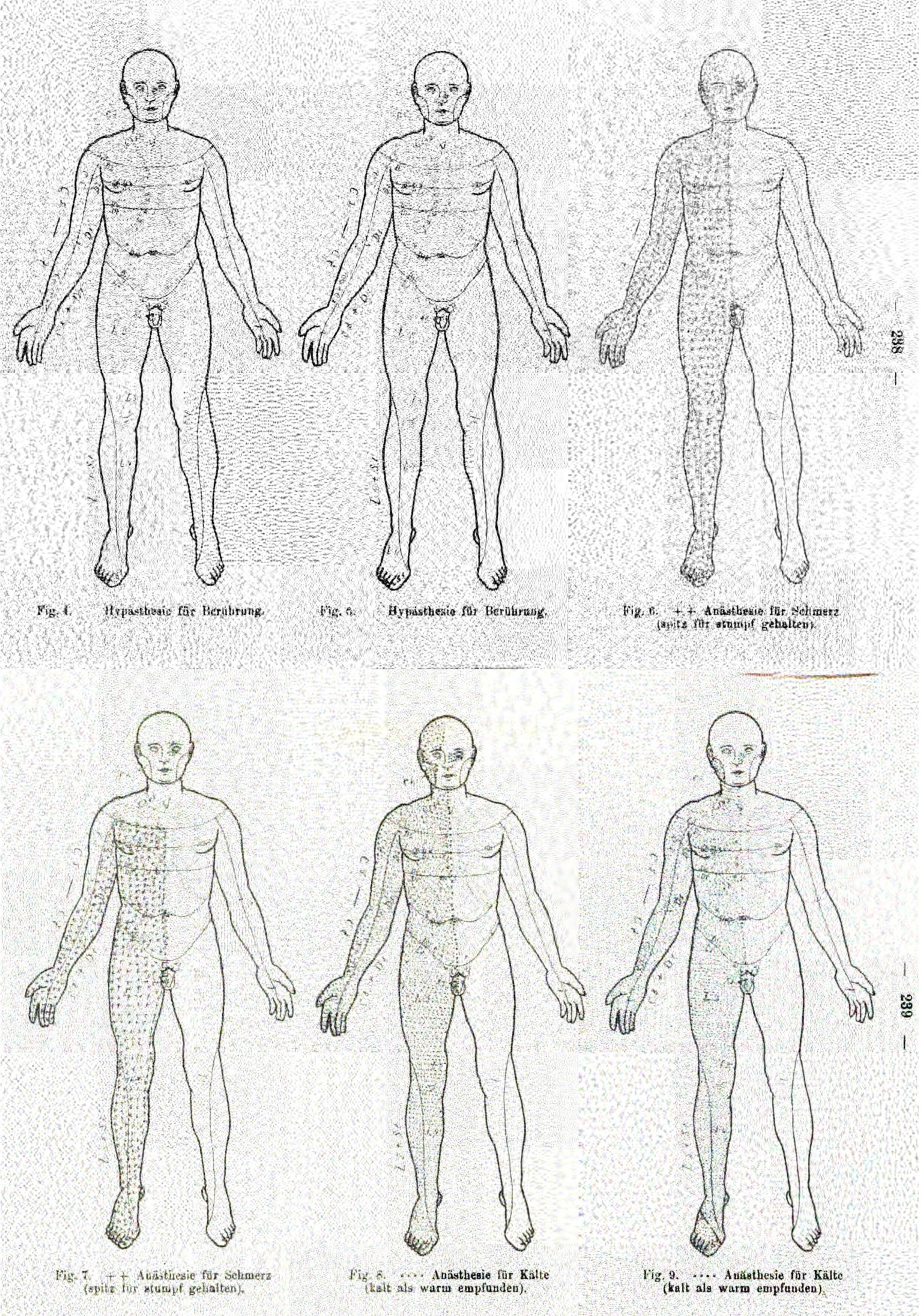
Wallenberg’s initial description of Wallenberg Syndrome. Wallenberg 1895; Acute Bulbäraffection (Embolie der Arteria cerebelli posterior inferior sinistra?), p. 516-518.
Two to three months after the attack, the patient’s status was as follows:
Subjective symptoms:
1. Dizziness, with a tendency to fall to the left.
2. Numbness in the left half of the face, and the right half of the body except for the face.
3. Difficulty swallowing (very minor).
4. Pain in the neck, sometimes in the left eye.
Objective symptoms:
1. Staggering to the left while walking.
2. Ataxia of the left extremities (only hinted at)
3. Paresis of the left soft palate.
4. Paralysis, later paresis of the left vocal cord (suggestion of atrophy?).
5. Larger volume of the left half of the tongue when the mouth is resting.
6. Sensitivity disturbance in the area of the first and second branch of the left trigeminal nerve, particularly affecting the eyes, lids, bridge of the nose, and nasal mucosa …
7. Absence of the left corneal and conjunctival reflex.
8. Disorders of the sensation of pain and coldness on the right half of the trunk …
9. Alterations of the other sensory qualities (namely localising sense, faradocutaneous sensitivity, sense of pressure) to a small extent …
10. Indication of ataxia of the left leg without disturbance of gross strength.
11. Absence of abdominal reflexes.
In the following weeks the swallowing difficulties gradually disappeared, the tendency to fall to the left, the ataxia; the other symptoms, namely the vocal cord, tongue and palate paresis and the sensory disorders remain essentially stationary. There is also a new symptom:
12. During auscultation of the right mastoid forties, a systolic sound can be traced backward to the grista occipitalis, downwards to the angle of the lower jaw, and forwards (albeit weakly!) to the temple. Pulsation of the neck vessels was stronger on the right than on the left.
Wallenberg’s initial description of Wallenberg Syndrome. Wallenberg 1895; Acute Bulbäraffection (Embolie der Arteria cerebelli posterior inferior sinistra?), p. 516-518
1901 – Wallenberg performed a post-mortem on the patient he reported on in 1894. He confirmed the exact anatomical location of the lesion to be in the posterior inferior cerebellar artery.
German
English
Die anatomische Untersuchung in einem Falle, bei welchem 6 Jabre vor dem Tode die Wahrscheinlichkeitsdiagnose einer Embolie der Art. cerebell. infer. post. sin. gestellt worden war, ergiebt einen Verschluss dieser Arterie durch einen Thrombus, von dem nicht mehr mit Sicherheit behauptet werden kann, ob er in loco entstanden ist oder aus der durch Arteriosklerose mit Thrombenbildung stark verengten Vertebralis sinistra stammt.
Wallenberg 1901; Anatomischer Befund in einem als ‘Akute Bulbäraffektion (Embolie der Art. cerebelli post. inf. sinister?)’ beschriebenen Fälle, p. 957-958.
The anatomical examination of the case, in which 6 years prior to death the probable diagnosis of an embolism of the posterior inferior cerebellar artery was made, showed this artery was indeed occluded by a thrombus, of which it can no longer be said with certainty whether it originated in situ or from the vertebralis sinistra, which is severely narrowed by arteriosclerosis with thrombus formation.
Wallenberg 1901; Anatomischer Befund in einem als ‘Akute Bulbäraffektion (Embolie der Art. cerebelli post. inf. sinister?)’ beschriebenen Fälle, p. 957-958.
1915 – Wallenberg published another case report on a 50-year old painter with a suspected left posterior inferior cerebellar artery. Wallenberg once again described many of the signs and symptoms he had seen in 1894.
1922 – Wallenberg published one final paper on the syndrome, this time detailing his 15th patient with the lesion and associated features. In this paper, he concluded that ‘on the basis of the deficit, it is possible to precisely demarcate the location and extent of a disease focus of the lateral oblongata down to a millimeter during life’.
1946 – Belgian neuropsychiatrist Denise Louis-Bar wrote a detailed analysis with an extensive bibliography on the lateral medullary syndrome. Her paper was the first to significantly eponymize Wallenberg to the syndrome.
Associated Persons
- Gaspard Vieusseux (1746-1814)
- Alexander Marcet (1770–1822)
- Hermann Senator (1834-1911)
- Adolf Wallenberg (1862-1949)
- Johann Friedrich Horner (1831 – 1886)
Alternative names
- Lateral medullary syndrome
- Viesseaux-Wallenberg syndrome
- Posterior inferior cerebellar artery syndrome (PICA)
References
Historical articles
- Marcet A. History of a singular Nervous or Paralytic Affection, attended with anomalous morbid sensations. Med Chir Trans. 1811;2:217–235.
- Senator H. Apoplectische Bulbärparalyse mit wechselständiger Empfindungslähmung. Archiv für Psychiatrie und Nervenkrankheiten. 1881;11:713-726
- Wallenberg A. Acute Bulbäraffection (Embolie der Arteria cerebelli posterior inferior sinistra?). Archiv für Psychiatrie und Nervenkrankheiten. 1895;27:504–540.
- Wallenberg A. Anatomischer Befund in einem als ‘Akute Bulbäraffektion (Embolie der Art. cerebelli post. inf. sinister?)’ beschriebenen Fälle. Archiv für Psychiatrie und Nervenkrankheiten. 1901;34:923–959.
- Wallenberg A. Verschluss der arteria cerebelli inferior posterior sinistra. Neurologische Zentralblatt. 1915;34:236–247
- Wallenberg A. Verschluss der arteria cerebelli inferior posterior dextra (mit sektionbefund). Deutsche Zeitschrift fur Nervenheilk. 1922;73:189–212.
Eponymous term articles
- Olivier, de Morsier. Le Dr. Gaspard Vieusseux (Genève 1746-1814) – La méningite cérébro-spinale. Le syndrome de Vieusseux-Wallenberg. Revue médicale de la Suisse romande 1943; 63: 421
- Louis-Bar D. Sur le syndrome vasculaire de l’hémibulbe (Wallenberg). Monatsschr Psychiatr Neurol. 1946;112(1-2):53-107.
- Pearce JM. Wallenberg’s syndrome. J Neurol Neurosurg Psychiatry. 2000 May;68(5):570.
- Hong YH et al. Lesion Topography and Its Correlation With Etiology in Medullary Infarction: Analysis From a Multi-Center Stroke Study in China. Front Neurol. 2018 Sep 27;9:813
- Hayes J. FFS: Lateral medullary syndrome. LITFL
eponymictionary
the names behind the name
Lewis is an RMO at Royal Perth Hospital. He is currently interested in critical care medicine.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |