
![]()
Adolf Wallenberg
Adolf Wallenberg (1862-1949) was a German internist and neurologist.
A resilient man, Wallenberg did not allow a base of skull injury or his service in the German army during World War I to impede his progress in the field of neurology, going on to become known worldwide by the top neurologists of his time. He published sixty-seven works before retirement, published the Bericht über die Leistungen auf dem Gebiete der Anatomie des Centralnervensystems in dem Jahren and described the avian brain alongside Ludwig Edinger, and received the Erb Medal in 1929 for his contributions.
Highly sought after, Wallenberg turned down teaching positions in various places, preferring to stay in his home country. However, the implemented Nazi regime saw Wallenberg stripped of his research laboratory and forced him to stop working due to being Jewish, and resulted in him emigrating to England, then the United States.
Wallenberg is eponymously affiliated with Wallenberg Syndrome and Wallenberg’s Tract. An annual prize awarded by the German Neuroscience Society since the 1980s for research excellence in the field of cerebrovascular diseases, cerebral blood flow, or brain metabolism is also named after him.
Biography
- Born November 10, 1862 Starogard Gdański, Poland son of the district’s physician Samuel Wallenberg
- Circa 1882 – Studied Medicine in Heidelberg under the guidance of teachers including Wihelm Erb, Adolf Strümpell, and Carl Weigert
- 1886 – Doctorate from the University of Leipzig under Strümpell and Weigert. Dissertation on poliomyelitis
- 1886 – Internist at Städtisches Krankenhaus in Danzig
- 1891 – Sustained a base of skull fracture whilst horse riding. Suffered from diplopia and anosmia
- 1895 – First clinically described Wallenberg Syndrome
- 1896 – First described Wallenberg’s Tract whilst working with rabbit brains
- 1895-1928 – Editor of the Bericht über die Leistungen auf dem Gebiete der Anatomie des Centralnervensystems in dem Jahren alongside Ludwig Edinger
- 1901 – Anatomically defined Wallenberg Syndrome
- 1907-1928 – Appointed chief physician to the Danzig city hospital
- 1910 – Received professorship
- 1914 – Studied at the Institute of Biology on Heligoland
- 1914-1918 – Served in the German Army in WWI; served as a military physician and advisor to the 17th army.
- 1929 – Received the Erb Medal for his merits in the field of anatomy, physiology, and pathology of the nervous system.
- 1938 – Fled the Nazi invasion of Danzig through Holland and Belgium, retreating to Oxford where he taught clinical neurology with neuroanatomist LeGros Clark
- 1943 – Emigrated to the United States and took up residency lecturing at a state mental hospital near Chicago.
- Died April 10, 1949 in Manteno, Illinois, USA of ischemic heart disease
Medical Eponyms
Wallenberg Syndrome (1894)
Also known as lateral medullary syndrome or the posterior inferior cerebellar artery syndrome.
A neurological disorder with a variety of symptoms associated with posterior circulation ischemic stroke. Signs include dizziness/vertigo, loss of balance with gait instability, hoarse voice and difficulty swallowing.
First described by Gaspard Vieusseux in 1808 where he recorded a detailed description of his own illness at a meeting of the Société médicochirugicale de Genève.
Wallenberg first reported on the syndrome in 1894 (published in 1895), where he intricately detailed the clinical findings of a 38-year old man with the syndromic features. His findings, alongside a detailed examination of seven brains, and the anatomical work of Henri Duret (1849-1921), allowed him to accurately localise the site of the lesion.
German
English
Zwei bis drei Monate nach dem Insult etwa folgender Status:
Subjective Symptome:
1. Schwindel, Neigung nach links zu fallen.
2. Taubheitsgefühl in der linken Gesichtshälfte, rechten Körperhälfte mit Ausnahme des Gesichtes.
3. Schluckbeschwerden (sehr gering).
4. Schmerzen im Nacken, zuweilen auch im linken Auge.
Objective Symptome:
1. Schwanken nach links beim Gehen.
2. Ataxie der linken Extremitäten (nur noch angedeutet).
3. Parese der linken Gaumensegelhälfte.
4. Paralyse, später Parese des linken Stimmbandes (Andeutung von Atrophie?).
5. Grösseres Volumen der linken Zungenhälfte bei ruhiger Lage im Munde.
6. Sensibilitätsstörung im Bereiche des ersten, weniger des zweiten Astes des linken Trigeminus, namentlich Auge, Lider, Nasenrücken und Nasenschleimhaut betreffend…
7. Fehlen des linken Comeal- und Conjunctivalreflexes.
8. Störungen des Schmerzund Kältegefühls an der rechten Rumpfhälfte…
9. Alterationen der übrigen Empfindungsqualitäten (namentlich Ortssinn, faradocutane Sensibilität, Drucksinn) in geringem Grade…
10. Andeutimg von Ataxie des linken Beines ohne Störung der groben Kraft.
11. Fehlen der Bauchreflexe.
In den folgenden Wochen verschwinden allmälig die Schluckbe-schwerden, die Neigung nach links zu fallen, die Ataxie; die anderen Erscheinungen, namentlich die Stimmband-, Zungen-, Gaumenparese und die SensibilitätsstOrungen bleiben im Wesentlichen stationär. Dazu gesellt sich ein neues Symptom:
12. Bei der Auscultation des rechten Warzenfortsaties systolisches Geräusch, das sich nach hinten bis zur Grista occipitalis, nach unten bis zum Unterkieferwinkel, nach vorne (sehr schwach!) bis zur Schläfe verfolgen lässt. Pulsation der Halsgefässe rechts stärker als links.
Wallenberg’s initial description of Wallenberg Syndrome. Wallenberg 1895; Acute Bulbäraffection (Embolie der Arteria cerebelli posterior inferior sinistra?), p. 516-518.
Two to three months after the attack, the patient’s status was as follows:\
Subjective symptoms:
1. Dizziness, with a tendency to fall to the left.
2. Numbness in the left half of the face, and the right half of the body except for the face.
3. Difficulty swallowing (very minor).
4. Pain in the neck, sometimes in the left eye.
Objective symptoms:
1. Staggering to the left while walking.
2. Ataxia of the left extremities (only hinted at)
3. Paresis of the left soft palate.
4. Paralysis, later paresis of the left vocal cord (suggestion of atrophy?).
5. Larger volume of the left half of the tongue when the mouth is resting.
6. Sensitivity disturbance in the area of the first and second branch of the left trigeminal nerve, particularly affecting the eyes, lids, bridge of the nose, and nasal mucosa …
7. Absence of the left corneal and conjunctival reflex.
8. Disorders of the sensation of pain and coldness on the right half of the trunk …
9. Alterations of the other sensory qualities (namely localising sense, faradocutaneous sensitivity, sense of pressure) to a small extent …
10. Indication of ataxia of the left leg without disturbance of gross strength.
11. Absence of abdominal reflexes.
In the following weeks the swallowing difficulties gradually disappeared, the tendency to fall to the left, the ataxia; the other symptoms, namely the vocal cord, tongue and palate paresis and the sensory disorders remain essentially stationary. There is also a new symptom:
12. During auscultation of the right mastoid forties, a systolic sound can be traced backward to the grista occipitalis, downwards to the angle of the lower jaw, and forwards (albeit weakly!) to the temple. Pulsation of the neck vessels was stronger on the right than on the left.
Wallenberg 1895; Acute Bulbäraffection (Embolie der Arteria cerebelli posterior inferior sinistra?), p. 516-518.
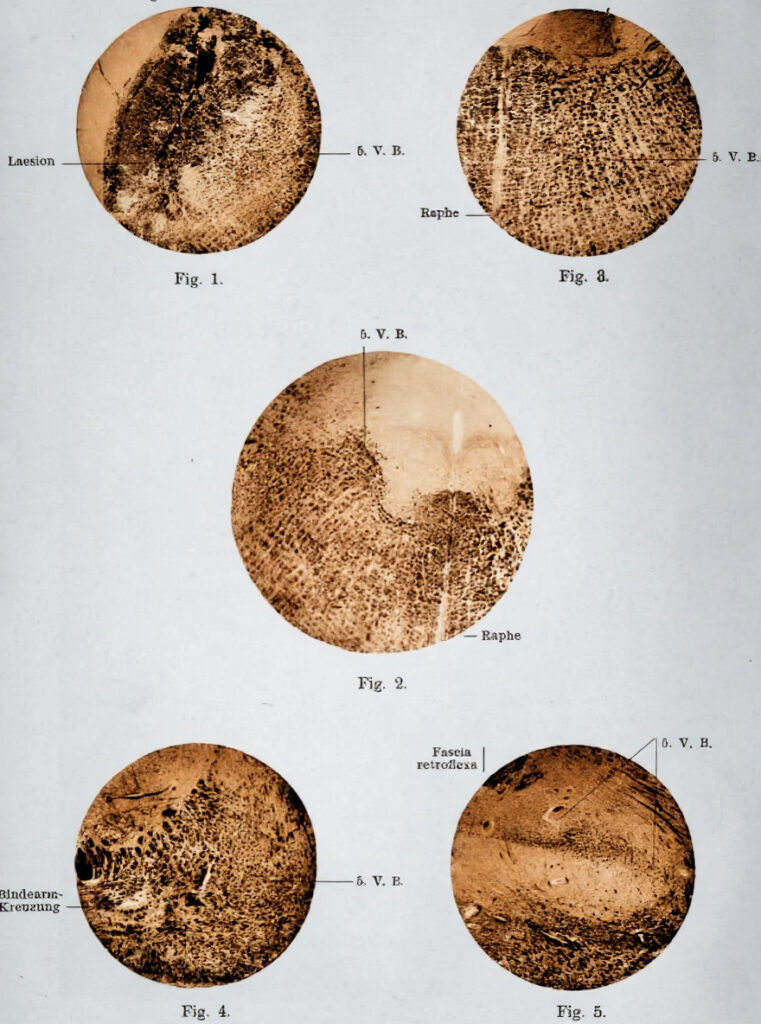
After the patient had passed away, Wallenberg was able to perform a post-mortem and confirm the exact anatomical location of the lesion in 1901.
German
English
Die anatomische Untersuchung in einem Falle, bei welchem 6 Jabre vor dem Tode die Wahrscheinlichkeitsdiagnose einer Embolie der Art. cerebell. infer. post. sin. gestellt worden war, ergiebt einen Verschluss dieser Arterie durch einen Thrombus, von dem nicht mehr mit Sicherheit behauptet werden kann, ob er in loco entstanden ist oder aus der durch Arteriosklerose mit Thrombenbildung stark verengten Vertebralis sinistra stammt.
Wallenberg 1901; Anatomischer Befund in einem als ‘Akute Bulbäraffektion (Embolie der Art. cerebelli post. inf. sinister?)’ beschriebenen Fälle, p. 957-958.
The anatomical examination of the case, in which 6 years prior to death the probable diagnosis of an embolism of the posterior inferior cerebellar artery was made, showed this artery was indeed occluded by a thrombus, of which it can no longer be said with certainty whether it originated in situ or from the vertebralis sinistra, which is severely narrowed by arteriosclerosis with thrombus formation.
Wallenberg 1901; Anatomischer Befund in einem als ‘Akute Bulbäraffektion (Embolie der Art. cerebelli post. inf. sinister?)’ beschriebenen Fälle, p. 957-958.
Wallenberg went on to publish two more papers detailing the syndrome; one in 1915 on a single case, and another in 1922 on his 15th patient with the syndromic features.
Wallenberg Tract (1896)
A dorsal trigeminal tract believed to be involved in the mediation of taste and tactile discrimination. Consists of two parts; a crossed tract arising from the descending branch nucleus and an uncrossed tract from the main sensory nucleus of the trigeminal nerve.
Wallenberg first described the tract in his 1896 paper, Die sekundiire Bahne des sensibelen Trigeminus, where he examined the brains of rabbits. He subsequently authored two more papers on the matter; one in 1900 and the other in 1905.
The existence of the tract was a matter of debate for a period after Wallenberg’s publications. However in 1960, neuropsychiatrist Willem Verhaart (1889-1893) was able to identify that the tract was conspicuous in certain mammals, but morphologically insignificant and subsequently absent in other mammals.
Major Publications
- Wallenberg A. Anatomischer Befund in einem als ‘Akute Bulbäraffektion (Embolie der Art. cerebelli post. inf. sinister?)’ beschriebenen Fälle. Archiv für Psychiatrie und Nervenkrankheiten. 1901;34:923–959. [Wallenberg Syndrome]
- Wallenberg A. Acute Bulbäraffection (Embolie der Arteria cerebelli posterior inferior sinistra?). Archiv für Psychiatrie und Nervenkrankheiten. 1895,27:504–540. [Wallenberg Syndrome]
- Wallenberg A. Die sekundiire Bahne des sensibelen Trigeminus. Anat Anz. 1896;12:95-110 [Wallenberg’s Tract]
- Wallenberg A. Sekundire sensibele Bahnen im Gehirnstamme des Kaninchen, ihre gegenseitige Lage und ihre Bedeutung fur den Aufbau des Thalamus. Anat Anz. 1900;18:81-105.
- Wallenberg A. Sekundiire Bahnen aus dem frontalen sensibelen Trigeminuskerne des Kaninchens. Anat Anz. 1905;26:145-155
- Edinger L, Wallenberg A. Bericht über die Leistungen auf dem Gebiete der Anatomie des Centralnervensystems. Leipzig: S.Hirzel 1907.
- Edinger L, Wallenberg A. Anatomie des Zentralnervensystems. Bonn: A. Marcus & E. Weber 1913.
- Wallenberg A. Verschluss der arteria cerebelli inferior posterior sinistra. Neurologische Zentralblatt. 1915;34:236–247
- Wallenberg A. Verschluss der arteria cerebelli inferior posterior dextra (mit sektionbefund). Deutsche Zeitschrift fur Nervenheilk. 1922;73:189–212.
References
Biography
- Wallenberg-Chermak M (1963) Adolf Wallenberg (1862–1949). In: Kolle K (ed) Grosse Nervenärzte. 1963; 3: 184–190.
- Hydén D, Norrving B. Adolf Wallenberg (1862–1949). J Neurol. 2005; 252: 1135–1136.
- Shoja MM, Tubbs RS, Loukas M, Ardalan MR. Adolf Wallenberg (1862-1949): physician and neuroanatomist. Childs Nerv Syst. 2008; 24(9): 979-981.
- Zeidman LA, Mohan L. Adolf Wallenberg: giant in neurology and refugee from Nazi Europe. J Hist Neurosci. 2014;23(1):31-44
- Fresquet JL. Adolf Wallenberg (1862-1949). Historia de la Medicina.
- Bibliography. Wallenberg, A. WorldCat Identities
Wallenberg Syndrome
- Pearce JM. Wallenberg’s syndrome. J Neurol Neurosurg Psychiatry. 2000 May;68(5):570.
Wallenberg’s Tract
- Verhaart WJC. The Tractus Trigeminalis of Wallenberg. Acta Psychiatrica Scandinavica, 1954;29:269-279.
- Verhaart WJC, Busch HF. Wallenberg’s tract, the fasciculus tegmentalis dorsolateralis and Forel’s fasciculi tegmentales. Acta Anat (Basel). 1960;40:41-58.
Eponym
the person behind the name
Lewis is an RMO at Royal Perth Hospital. He is currently interested in critical care medicine.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |