
![]()
William Ewart

William Ewart (1848-1929) was an English physician.
Ewart was skilful in the art of physical examination, especially in auscultation and percussion. He was a conscientious but eccentric teacher, alternating between brevity and diffuseness.
Whilst at the Brompton hospital he developed a significant interest in thoracic disease which, with climatological reports, was the principal subject of his writings
In his paper 1896 entitled “Practical aid in the diagnosis of pericardial effusion in connection with the question as to surgical treatment” described 12 signs of pericardial effusion, two of which bear his name: Ewart sign and Ewart sign II
Biography
- Born on December 26, 1848 in London; the son of an English father and French mother
- 1867 – Baccalauréat ès lettres, University of Paris
- 1869 – Medical school, St. George’s Hospital
- 1870 – Medical studies interrupted; medical officer with the French army
- 1871 – MB, LRCS, LRCP.
- 1875 – House physician, Addenbrooke’s Hospital, Cambridge; attended Gonville and Caius College.
- 1881 – FRCP, Fellow of the Royal College of Physicians; assistant physician and pathologist at the Hospital for Consumption and Disease of the Chest, Brompton
- 1882 – Doctor of medicine, Cambridge University; assistant physician at St. George’s hospital; presented the Goulstonian Lectures at the at the Royal College of Physicians
- 1887 – Full physician at St. George’s hospital
- 1894-1897 Examiner, Royal College of Physicians
- 1907 – Consulting physician at St. George’s hospital
- 1908 – Chairman of the British Medical Association, Westminster Division
- Died on August 11, 1929 in London
Medical Eponyms
In 1896 Ewart addressed the North London District of the Metropolitan branch of the British Medical Association. He advised that (1) accurate percussion (using Sansom’s pleximeter) and palpation; (2) careful auscultation; and (3) observation of the pulse were essential in determining the size of a pericardial effusion and raise the question as to surgical interference. He defined 12 signs of pericardial effusion, including what would later be termed Ewart sign (sign 8 and 10); and Ewart sign II (sign 7)
Ewart sign (1896)
In pericardial effusions, the presence of an area of variable size with dullness in the region of the inferior angle of the left scapula associated with a corresponding area of bronchial breathing, increased fremitus and aegophony (see also Pins sign I). Ewart attributed the signs to partial collapse of pulmonary tissue and pressure on a bronchus.
[Eighth sign] The Posterior Pericardial Patch of Dulness. A patch of marked dulness (Fig. 4) is found at the left inner base, extending from the spine for varying distances outwards, usually not quite so far as the scapular (angle) line, and ceasing abruptly with a vertical outer boundary. Above, its extension is also variable, according to the size of the effusion; commonly it does not extend higher than the level of the ninth or tenth rib, and here again its horizontal boundary is abrupt. Its shape then is that of a square, and it is quite unlike that of any dulness arising from pleuritic effusion. You will not experience any difficulty in identifying the patch in question.
[Tenth sign] The Posterior Pericardial Patch of Tubular Breathing and Aegophony: Immediately below or slightly to the left of the tip of the left scapula a patch about 2 inches in diameter presents well-marked tubular breathing and aegophony (see T; Ae in Fig. 4). This sign, although not so important as that of the patch of dulness, is very commonly, if not always, present in cases of considerable effusion, and gives valuable confirmation to other signs. It has been described by other observers (Bamberger 1857, Pins 1889).
Ewart 1896: 721
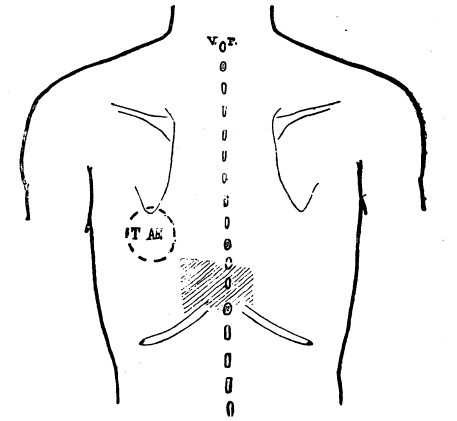
Ewart 1896: Fig 4. The ‘posterior pericardial patch of dulness’ (shaded); and T-Ae the ‘posterior pericardial patch of tubular breathing and aegophony’
Ewart sign II (1896)
A large pericardial effusion makes the first rib seem more prominent along the sternal border
[Seventh sign] The First Rib Sign. In all cases of considerable pericardial effusion which I have examined for this sign, it was possible to feel with the finger the upper edge of the first rib as far as its sternal attachment (see F in Fig. 3). This points to a raising of the clavicle not only in its outer but also in its inner portion; and to a relaxation of the ligament between it and the first rib. In the absence of pericardial effusion I have rarely seen this sign, except in some cases of considerable cardiac enlargement. I regard it as specially connected with the immobility and with the elevation of the lower ribs, coupled with the great activity of the superior respiratory region of the chest. The left clavicle is apparently lifted to a higher level than it is possible for the first rib to reach.
Ewart 1896: 720
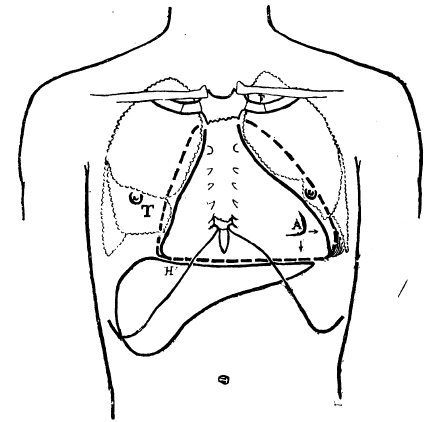
Ewart 1896: Fig. 3. Outlines of the total and of the absolute areas of pericardial dulness. (A) position of the cardiac apex (fifth space) in the effusion. The dulness is shown by the arrows to extend far beyond and below A; (F), the first rib sign (7th sign); (T), the inframammary patch of tubular breathing (9th sign).
Ewart’s twelve signs of pericardial effusion:
- Considerable Extension of the Lateral Boundaries of the Total area of Dulness
- Great Extension of the Absolute dulness; the sternum Absolutely Dull
- The Depression of the Liver
- Dulness in the Right Fifth Intercartilaginous Space [Rotch’s sign]
- The Diagnosis Between Pericardial Effusion and Cardiac Dilatation: The Lower Angle of the Pericardial Dulness projects towards the Right.
- The Left Lower Angle of Dulness. The Relation of the Apex Beat to this Angle
- The First Rib Sign [Ewart sign II]
- The Posterior Pericardial Patch of Dulness. [Ewart sign][Pins sign I]
- Tubular Breathing Below the Right Breast. Although not constant, this sign, which does not appear to have been noticed, should be looked for in severe cases.
- Posterior Pericardial Patch of Tubular Breathing and Aegophony [Ewart sign]
- Secondary Pleural Effusions
- The Large and Slapping Pulse of Pericardial Effusion. First mentioned in the light of a tactile hallucination ‘La Circulation du Sang‘ by Étienne-Jules Marey (1830-1904)
Controversies
Whilst Ewart worked in a field hospital during the Franco-Prussian War, he wrote of the German surgeons reluctance to operate “They were always anxious to give unaided nature her last chance, by which they often seemed to deprive the patient of his.” However, of the 14,000 amputations performed by French surgeons during the war, 10,000 died of sepsis…so it seems the German’s reluctance to operate was well founded.
Major Publications
- Ewart W. The future training of the medical profession. London: Harrison. 1888
- Ewart W. The bronchi and pulmonary blood-vessels. London: Churchill. 1889
- Ewart W. The value of accuracy in cardiac percussion. Lancet. 1891; 138(3548): 473-476 [Sansom’s pleximeter]
- Ewart W. Cardiac outlines for clinical clerks and practitioners. New York: Putnam. 1892
- Ewart W. How to feel the pulse and what to feel in it. New York: W. Wood. 1892
- Ewart W. The pulse-sensations: a study in tactile sphygmology. In: Heart studies, chiefly clinical London. 1894
- Ewart W. Practical aids in the diagnosis of pericardial effusion, in connection with the question as to surgical treatment. Br Med J. 1896;1:717-721. [Ewart sign]
- Ewart W. Grocco’s Paravertebral Triangle. Br Med J 1908; 2: 1896
- Ewart W. Gout and goutiness and their treatment. London: Baillière, Tindall and Cox. 1896
- Ewart W. Grocco’s triangle in pleural effusion. Lancet. 1905; 166(4274): 316
- Ewart W. Marine climates in the treatment of tuberculosis. London: Baillière, Tindall and Cox. 1907
- Ewart W. “Res medica, res publica”: the profession of medicine, its future work and wage. 1907
References
Biography
- Obituary: William Ewart, M.D., F.R.C.P. Br Med J 1929; 2: 369
- Obituary: William Ewart. Lancet. 1929; 214(5530): 408–409
- Biography: William Ewart. Lives of the Fellows of the Royal College of Physicians of London. Munk’s Roll: Volume IV: 280
- Bibliography. Ewart, William 1848-1929. WorldCat Identities
Eponymous terms
- Babcock RH. Pericarditis with effusion. In: Diseases of the heart and arterial system. 1907: 80-81
- Musser JH. Practical Treatise on Medical Diagnosis for Students and Physicians, 1894: 397 and 1913: 615.
- Christian HA. The frequency of pulmonary compression signs in acute fibrinous pericarditis. JAMA. 1918; 71(6):419-422.
- Conner LA. On the diagnosis of pericardial effusion: With special reference to physical signs on the posterior aspect of the thorax. American Heart Journal. 1926; 1(4): 421–433
- Steinberg I. Pericarditis with effusion: new observations, with a note on Ewart’s sign. Ann Intern Med. 1958 Aug;49(2):428-37.
- Sartawi T, Warner C, White P. Point-of-care ultrasound evaluation in cardiac tamponade: first description of a ‘sonographic Ewart’s sign‘ Chest. 2019; 156(4): S
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |