
![]()
Activate or Wait – 007
84 year-old woman from home with central chest pain following a fall. Background of hypertension and dyslipidaemia.
ETA 20 minutes to your tertiary centre.

Would you activate your cath lab/STEMI protocol?
0
ECG interpretation
Anterolateral OMI
- Diffuse ST elevation globally in leads I, II, III, aVF, V2-V6
- Reciprocal ST depression in aVR
- PR depression, ST elevation in II > III, and ST segments almost as tall as T waves are all typical of pericarditis. However, one would never dare diagnose pericarditis in an 84-year-old with ST elevation
AI interpretation by PMcardio
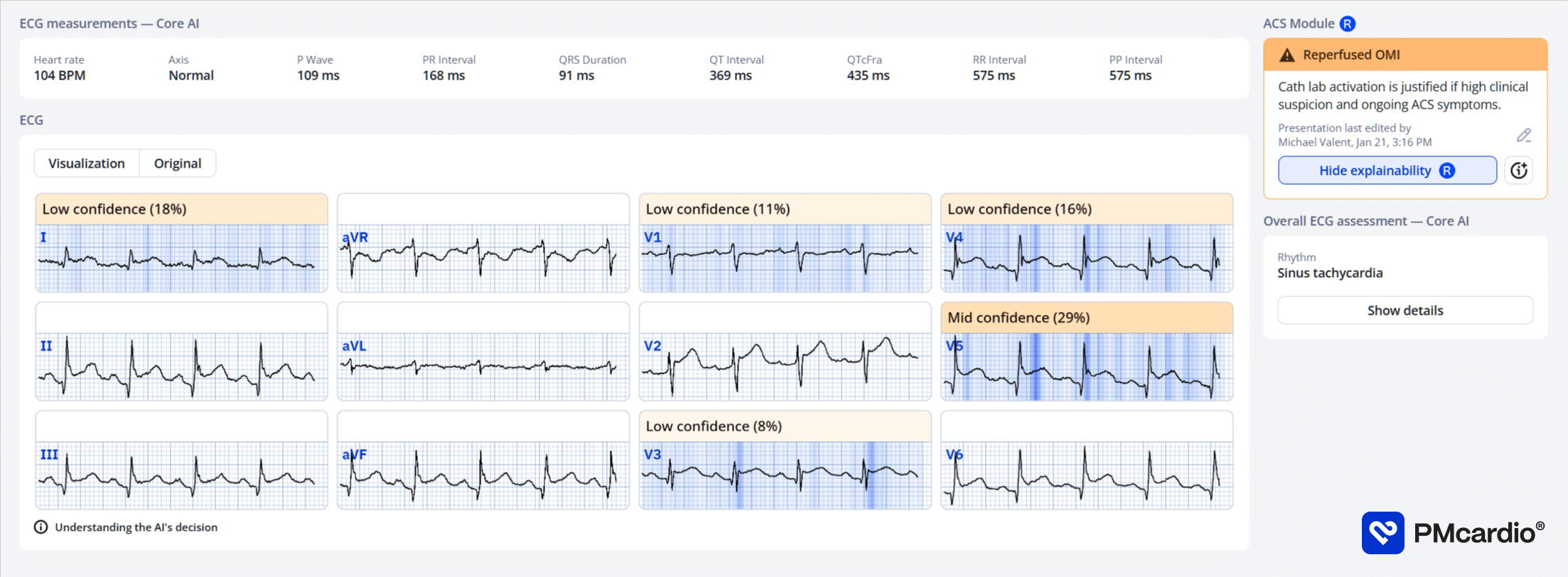
PMcardio’s AI ECG model identified a Reperfused OMI.
The explainability feature offers insights into problematic patterns in the respective leads, providing a clear rationale for the diagnosis.
Further reading
Outcome
The patient was taken for emergent angiography upon arrival.
Key Finding:
Takotsubo cardiomyopathy
Findings:
- Left Main Coronary Artery – large calibre, very short.
- Left Anterior Descending Coronary Artery – medium calibre, calcified moderate 40% disease at bifurcation of D1.
- Left Circumflex Coronary Artery – non-dominant, medium calibre, mild disease.
- Right Coronary Artery – dominant, medium calibre, moderate 60% calcified eccentric disease in mid vessel.
- Left Ventriculogram – Apical hypo-akinesis with basal hyperkinesis
Plan:
- Takotsubo cardiomyopathy with moderate, nonobstructive coronary artery disease.
- Ongoing medical therapy and risk factor modification
- Admit to CCU
Clinical Pearls
Takotsubo cardiomyopathy, or ‘broken-heart syndrome’, describes transient dyskinesis of the left ventricular wall, often occurring in the context of severe emotional or physical stress. It presents with ischaemic chest pain, a troponin elevation and ECG changes that mimic a STEMI.
Coronary angiography is necessary to differentiate the two conditions.
A pericarditis ECG pattern in an elderly patient should always prompt consideration of acute coronary occlusion and angiography, regardless of how typical the ECG features appear.
References
Further reading
- Buttner R, Burns E. Takotsubo Cardiomyopathy. LITFL
- Burns E, Buttner R. The ST Segment. LITFL
- Nickson C. STEMI Management. LITFL
Online resources
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Smith SW. Dr Smith’s ECG blog.
- Rawshani A. Clinical ECG Interpretation ECG Waves
ACTIVATE or WAIT
EKG Interpretation

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Dr. Stephen W. Smith is a faculty physician in the Emergency Medicine Residency at Hennepin County Medical Center (HCMC) in Minneapolis, MN, and Professor of Emergency Medicine at the University of Minnesota. Author of Dr Smith's ECG Blog | Bibliography | X |

Dr. Robert Herman is the Co-founder and Chief Medical Officer of PMcardio by Powerful Medical. He is a cardiovascular researcher at the Cardiovascular Center Aalst in Belgium, specializing in applying AI to enhance the detection and referral of cardiovascular patients. LinkedIn | X (formerly Twitter) | Get in Touch

PR depression?
Looked like Spodick sign to me…