
![]()
Bronchoscopic Foreign Body Removal
Flexible bronchoscopy is first‑line in most adults (>90% success) for airway foreign body removal, while rigid bronchoscopy remains essential for large, sharp, proximal, or asphyxiating objects.
See Airway Foreign Bodies for causes, pathophysiology, complications, clinical features, investigations, and management overview.
INDICATIONS FOR BRONCHOSCOPY
Flexible bronchoscopy is usually first line for most AFB situations:
- CT shows AFB
- CT negative but suspicion high
- Persistent unexplained respiratory symptoms
- Recurrent same‑lobe infection
- Localised wheeze or obstruction
However, flexible bronchoscopy should not be performed if indications for rigid bronchoscopy are present:
- Asphyxiating FBs
- Large objects (>1.5 cm diameter)
- Sharp objects
- Proximal tracheal/ main bronchial AFB
- Massive bleeding
- Failed flexible bronchoscopy
PRE‑PROCEDURAL PLANNING
Assess:
- the AFB
- Size
- Shape
- Substance
- Site
- the patient
- Oxygenation, ventilation
- Airway anatomy
- Comorbidities
- Anaesthesia tolerance (including allergies and airway reactivity)
To inform the following plan:
- Imaging
- CT is ideal for localisation and assessing granulation, but not always feasible in unstable patients or required in children where radiation exposure is of greater concern
- Flexible versus Rigid Bronchoscopy
- Rigid: asphyxiating FBs, large/sharp/impacted objects, need for ventilation control.
- Flexible: stable patients, distal FBs, diagnostic evaluation.
- Many cases benefit from combined use (flexible through rigid barrel).
- Primary Airway Device
- Not required for awake bronchoscopy with topical anaesthesia
- SGA (LMA): allows oxygenation during flexible bronchoscopy; useful in children.
- ETT: protects airway but may limit instrument size; often removed for rigid bronchoscopy.
- Rigid barrel: best for control, ventilation, and tool access.
- Primary and Backup Tools
- Primary: forceps, baskets, cryoprobe, Fogarty balloon.
- Backup: electrocautery, suction catheters, secondary forceps sizes.
- Ensure all tools match the working channel of the chosen scope.
- Backup Airway Plans
- Which techniques are likely to be effective?
- FMV (bag‑mask ventilation), SGA insertion, ETT intubation, FONA (front‑of‑neck access) for “can’t intubated, can’t oxygenate” (CICO)
- Rigid bronchoscopy should always be available when flexible bronchoscopy is attempted for FB extraction
- Which techniques are likely to be effective?
FLEXIBLE VERSUS RIGID BRONCHOSCOPY
Flexible bronchoscopy advantages
- High success rate (~90%) for FB retrieval
- Excellent for small/ smooth/ peripheral FBs
- Widely available in almost all hospitals
- No need for general anaesthesia in many cases
- Excellent access to distal airways
- Can be used through an ETT or LMA
- Lower desaturation risk during the procedure
- Allows granulation tissue removal and inspection for fragments
Flexible bronchoscopy disadvantages
- Limited airway protection
- Limited bleeding control
- Loss of airway possible during extraction
- Not suitable for some FBs (see below for rigid bronchoscopy indications)
- Does not provide a secure airway (unless intubated and ETT is not removed)
- Limited ability to control major bleeding
- Cannot reliably protect vocal cords from sharp objects
- Smaller working channel means can only use smaller tools
- Risk of losing the object during extraction through the glottis or ETT
- Less safe or effective for large, sharp, or impacted objects
Rigid bronchoscopy advantages
- gold standard for large, sharp, or proximal AFBs
- Provides a stable, protected airway
- Better control of bleeding (tamponade, large suction) – preferred in massive haemorrhage or airway trauma
- Allows use of larger, stronger retrieval tools
- Protects vocal cords when removing sharp objects
- Allows flexible bronchoscope to be used through the barrel
Rigid bronchoscopy disadvantages
- Requires general anaesthesia
- Limited availability (equipment + expertise)
- Cannot reach distal airways
- More technically demanding
- Not suitable in some anatomies (retrognathia, cervical immobilisation)
- Risk of dental or glottic injury
| Feature | Flexible Bronchoscopy | Rigid Bronchoscopy |
|---|---|---|
| Airway control | Poor – no secure airway | Excellent – stable, protected airway |
| Anaesthesia | Often no GA required | Requires general anaesthesia |
| Access | Excellent for distal airways | Limited to central airways |
| Tool size / strength | Small working channel; smaller tools | Large, strong tools; better grip |
| Bleeding control | Limited | Excellent (tamponade, large suction) |
| Sharp object protection | Poor | Excellent – protects vocal cords |
| Large object removal | Difficult | Ideal |
| Availability | Widely available | Limited to specialist centres |
| Operator skill | Moderate | High; specialised training |
| Use in trauma | Good for distal debris, clots | Best for bleeding, teeth, shrapnel |
| Risk profile | Loss of airway, object dislodgement | Dental/glottic injury; more invasive |
| Success rate | ~90% for adult FB retrieval | Highest success for complex FBs |
RETRIEVAL TOOLS & TECHNIQUES
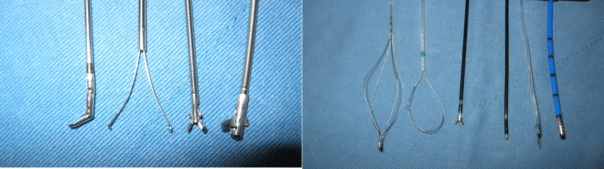
Figure. Examples of retrieval tools for flexible bronchoscopy, including forceps (e.g. two-prong, alligator, rubber tip), Dormia basket, snare or loop, coagulation forceps, coagulation knife, and probe for cryotherapy. Image from Fang et al (2015), available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC4358882/
| Tool | Best For | Technique | Notes |
|---|---|---|---|
| Forceps | Metal, bone, dentures, sharp objects | grasp edge → twist/rock → withdraw as single unit | Types: standard biopsy, rat‑tooth, shark‑tooth, alligator, rubber‑tipped |
| Snare | Large, rigid, irregular objects (broncholiths, dental prostheses) | open loop → abut → angle → tighten → extract | Excellent for bulky or irregular shapes |
| Basket | Smooth, round objects (peanuts, seeds, beads) | pass beyond → open → cage → tighten → withdraw | Avoid excessive traction to prevent fragmentation |
| Balloon catheter (Fogarty) | Distal or impacted objects; objects with central lumen | pass beyond → inflate with saline → pull proximally | Useful for dislodgement prior to forceps extraction |
| Cryoprobe | Semisolid, water‑rich material (blood clots, mucus plugs, food slurry) | freeze to –20°C → ice adhesion → withdraw en bloc | Avoid in active bleeding (risk of mucosal adhesion) |
Type of FB matched to tool
- Graspable FB: serrated rigid forceps / rat‑tooth forceps.
- Smooth/rounded FB: basket or fish‑net forceps.
- Organic FB: cryoprobe (“adheres the object to the frozen probe tip”).
- Impacted FB: Fogarty balloon.
- Sharp FB: fine grasping forceps with withdrawal into rigid barrel.
- Granulation‑covered FB: electrocautery debridement.
- Large objects FB: en bloc removal of bronchoscope, forceps, and FB.
CRITICAL CARE SCENARIOS
Common types of FB and typical scenarios encountered in critical care:
| Type of FB | Typical Scenario | Best Tool / Approach |
|---|---|---|
| Blood clots | Haemorrhage, anticoagulation, post‑procedure bleeding, pulmonary contusion (trauma) | Suction, forceps, cryoprobe |
| Mucus plugs | Prolonged ventilation, weak cough, dehydration, neuromuscular disease, rib fractures | Suction ± cryo, lavage |
| Aspirated food or gastric contents | Reduced consciousness, vomiting during intubation, TBI, intoxication | Basket or forceps; flexible bronchoscopy first |
| Teeth and dental fragments | Facial trauma, difficult intubation, maxillofacial fractures | Forceps; CT localisation helpful |
| Iatrogenic airway fragments | ETT cuff rupture, suction catheter tips, bite block fragments, bronchoscopy tool failure | Forceps or snare |
| Tracheostomy‑related debris | Broken inner cannula, valve components, gauze, secretions | Forceps; suction; consider rigid if large |
| Burn or inhalation injury debris | Soot, sloughed mucosa, fibrin casts in thermal/smoke injury | Suction, lavage, cryo for adherent debris |
| Penetrating trauma fragments | Bullet/shrapnel fragments, bone splinters, glass | Snare or rigid bronchoscopy |
| Broncholiths or calcified material | Chronic infection (TB, histoplasmosis), lymph node erosion | Snare or forceps |
| Large obstructing casts | Plastic bronchitis, inhalation injury, severe inflammation | Cryoextraction or basket |
Ready to check if these new guidelines have stuck?
Try these questions complete with answers and explanations.
References and Links
LITFL CCC
Journal articles
- Chi J, Bai Y. Bronchoscopic management of airway foreign bodies in adults: a narrative educational review. Front Med (Lausanne). 2026 Mar 4;13:1779715. doi: 10.3389/fmed.2026.1779715. PMID: 41859138; PMCID: PMC12996173.
- Fang YF, Hsieh MH, Chung FT, Huang YK, Chen GY, Lin SM, Lin HC, Wang CH, Kuo HP. Flexible bronchoscopy with multiple modalities for foreign body removal in adults. PLoS One. 2015 Mar 13;10(3):e0118993. doi: 10.1371/journal.pone.0118993. PMID: 25768933; PMCID: PMC4358882.
- Goyal R, Sehgal IS, Agarwal R. Foreign body removal. Curr Opin Pulm Med. 2026 Jan 1;32(1):63-73. doi: 10.1097/MCP.0000000000001225. Epub 2025 Oct 10. PMID: 41076577.
- Hewlett JC, Rickman OB, Lentz RJ, Prakash UB, Maldonado F. Foreign body aspiration in adult airways: therapeutic approach. J Thorac Dis. 2017 Sep;9(9):3398-3409. doi: 10.21037/jtd.2017.06.137. PMID: 29221325; PMCID: PMC5708401.

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC