
![]()
CICM SAQ 2011.2 Q9
Questions
9.1 The following arterial blood gas and biochemistry results are from a patient with cardiac and respiratory disease and recent profuse vomiting
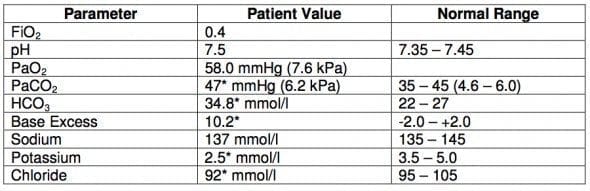
- a) Describe the acid-base disturbance(s)
- b) List the potential causes of the acid-base abnormalities in this patient
9.2 A 35-year-old woman with pre-eclampsia is admitted to ICU following an emergency Caesarian section under general anaesthesia for failure to progress during labour at 38 weeks gestation. Arterial blood gas, full blood count and electrolytes post extubation are as follows:

- a) Describe and explain the acid-base status
- b) Calculate and interpret the A-a gradient
- c) What is the likely significance of the anaemia and the leukocytosis?
Answers
Answer and interpretation
9.1 a) Describe the acid-base disturbance(s)
- Metabolic alkalosis with respiratory compensation
9.1 b) List the potential causes of the acid-base abnormalities in this patient
Possible causes in this patient:
- Diuretic therapy
- Steroid therapy
- Vomiting from gastric outlet obstruction Post hypercapnoeic alkalosis
9.2 a) Describe and explain the acid-base status
- Acute respiratory acidosis
- At 38 weeks pregnancy the normal PaCO2 is <30 mmHg with a compensatory reduction in bicarbonate. The blood gases therefore indicate acute CO2 retention probably due to pain and narcotics. In the non-pregnant patient these results would indicate an uncompensated normal anion gap metabolic acidosis.
9.2 b) Calculate and interpret the A-a gradient
- A-a gradient – this is raised at 154 mmHg, suggesting shunt and/or V/Q mismatch.
- Possible explanations are the loss of FRC after abdominal surgery, segmental collapse/consolidation or aspiration
9.2 c) What is the likely significance of the anaemia and the leukocytosis?
- Hb and WCC – the mild anaemia is physiological in pregnancy and the neutrophil leukocytosis is a normal feature during labour and early post-partum

Examination Library
CICM
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
