
![]()
CICM SAQ 2012.1 Q8
Questions
a) A 74-year-old man with known ischaemic heart disease was admitted to hospital for treatment of worsening heart failure (day 1). Despite treatment for heart failure he failed to improve and was referred for urgent intensive care assessment on day 5.
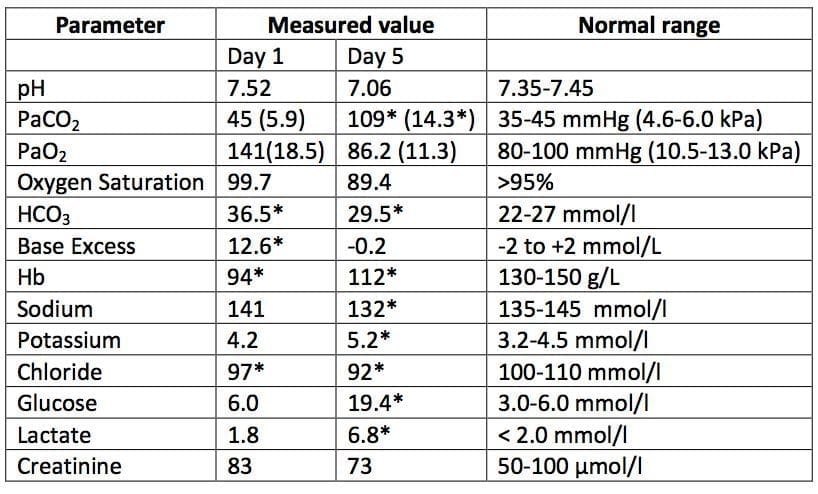
- i. Describe the acid-base abnormality on the Day 1 blood gas and give a clinical explanation that most likely caused this picture
- ii. Describe the acid-base abnormality on the Day 5 blood gas and give three possible clinical explanations
b) A 67-year-old lady is transferred from a regional hospital to a tertiary referral centre with a diagnosis of septic shock from a urinary source. She has not improved despite 48 hours of treatment with antibiotics and supportive care.

- i. Describe her biochemical profile on admission
- ii. List the causes of a raised lactate in sepsis
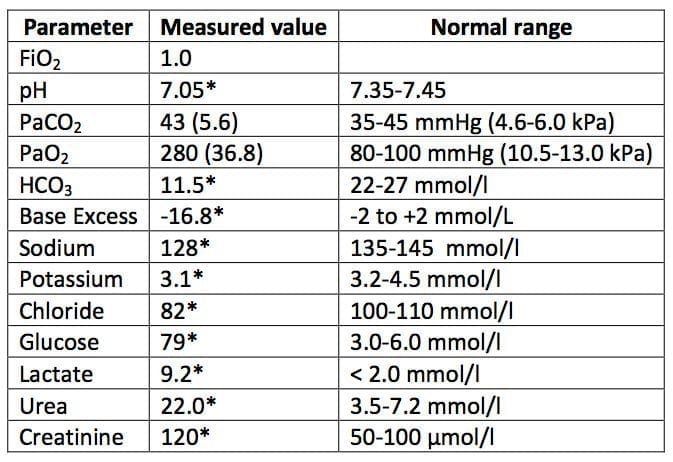
c) A 75-year-old woman with a reduced level of consciousness is intubated and ventilated following a single grand mal convulsion.
List the pathophysiological disturbances revealed by the following arterial blood gas and electrolyte profile taken 10 mins after intubation and give the likely explanation.
Answers
Answer and interpretation
a) i. Describe the acid-base abnormality on the Day 1 blood gas and give a clinical explanation that most likely caused this picture
- Chronic metabolic alkalosis with partial respiratory compensation
- Background of chronic metabolic alkalosis with partial respiratory compensation could be due to diuretic therapy for heart failure (“contraction alkalosis”)
a) ii. Describe the acid-base abnormality on the Day 5 blood gas and give three possible clinical explanations
- Superimposed acute respiratory acidosis and metabolic acidosis (raised lactate)
- Concomitant metabolic alkalosis given that the acidosis is not severe for the degree of PCO2 and lactate + BE is normal for the lactate + AG is also normal.
The acute superimposed pathology:
- Cardiogenic shock
- Sepsis
- Respiratory depression from opiate or illness
- PE
- Any other reasonable cause
b) i. Describe her biochemical profile on admission
- Mixed acidosis: Severe metabolic acidosis with a raised anion gap + additional respiratory acidosis
- Renal failure with hyponatraemia and hyperkalaemia
ii. List the causes of a raised lactate in sepsis
- Adrenaline
- Pyruvate dehydrogenase inhibtion by endotoxin
- Liver dysfunction/failure
- Tissue hypoxia
c) Pathological disturbances
- Uncompensated metabolic acidosis (or metabolic + respiratory acidosis) with raised anion gap not solely due to elevated lactate
- Raised A-a gradient
- Sodium adjusted to normoglycaemia is about 153
- Marked hyperglycaemia (candidates will say this but does not deserve a mark)
- Hyperosmolar hyperglycaemic syndrome with component of ketoacidosis and post-ictal lactic acidosis.

Examination Library
CICM
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
