
![]()
CICM SAQ 2013.2 Q7
Questions
7.1 A 65-year-old male has been brought into the Emergency Department after being found unconscious at home. He has a heart rate of 87 beats/min, a blood pressure of 96/59 mmHg, and temperature of 31.2oC.
Below is his biochemical profile and arterial blood gas analysis on a Hudson mask delivering 6 L/min oxygen:
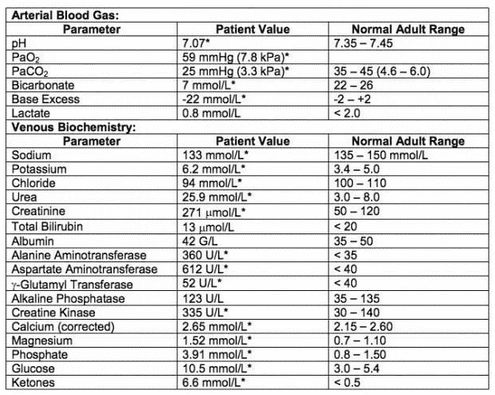
- a) Describe the acid-base abnormalities seen in the arterial blood gas analysis.
- b) List three possible causes of the ketosis.
- c) What is the most likely cause? Give your reasoning.
—
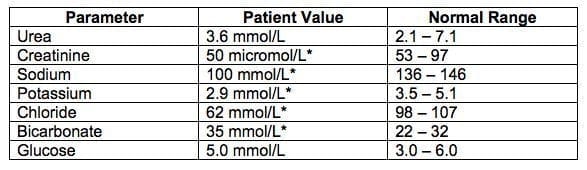
7.2 A 50-year-old Scottish male tourist presents with a three-day history of nausea, vomiting, general lethargy and dizziness. He had similar symptoms one year previously while on holiday in Cyprus and has had multiple presentations to his GP since then with general lethargy and weight loss.
The results of his investigations are as follows:

- a) What is the likely diagnosis?
- b) What investigation would you order to confirm your diagnosis?
—
7.3
A 61-year-old male, due to have a colonoscopy as an out-patient, is brought into the Emergency Department on the day of the procedure having been found collapsed at home, unresponsive with increased tone in his limbs.
- a) What is the likely cause of the biochemical disturbance?
- b) Briefly list the steps in your immediate management.
Answers
Answer and interpretation
7.1 a) Describe the acid-base abnormalities seen in the arterial blood gas analysisb) List three possible causes of the ketosisc) What is the most likely cause? Give your reasoning
a) Describe the acid-base abnormalities seen in the arterial blood gas analysis
- High anion gap metabolic acidosis (ketones and other unmeasured anion).
- Respiratory acidosis / inadequate respiratory compensation.
b) List three possible causes of the ketosis
- Alcoholic ketosis.
- Diabetic (euglycaemic) ketoacidosis.
- Starvation ketosis
c) What is the most likely cause? Give your reasoning.
- Alcoholic ketosis.
- Combination of severe AG acidosis with high level of ketones (too high for starvation ketosis) and abnormal liver enzymes (less likely with DKA).
7.2
a) What is the likely diagnosis?
- Hypoadrenalism or Addisonian crisis
b) What investigation would you order to confirm your diagnosis?
- Random cortisol
7.3
a) What is the likely cause of the biochemical disturbance?
- Water intoxication secondary to bowel prep.
b) Briefly list the steps in your immediate management.
- Airway control and treat seizures as indicated.
- Correct hypovolaemia [LITFL note: odd for water intoxicated patients to be hypovolemic?]
- Check serum osmolality (expected to be low).
- Hypertonic saline to increase [Na+] by approx. 0.5 mmol/L/hour to achieve safe level to limit seizures (> 118 mmol/L) – balance between gradual increase in sodium and achieving safe level to limit seizures.
- Correct hypokalaemia.
- Fluid restriction.
- Cease any medications that predispose to hyponatraemia (anti-depressants, thiazide diuretics, PPIs, ACEIs).
- CT brain to assess for cerebral oedema.

Examination Library
CICM
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
