![]()
CICM SAQ 2015.1 Q1
Question
You are called to review a 29-year-old male with confirmed asthma in the Emergency Department. He has been unwell for 2 days with increasing cough, wheeze and shortness of breath. He has just been intubated.
- a) Describe what ventilator settings you will initially set and give the reasons for your answer. (40% marks)
Two hours later he has become increasing difficult to ventilate. You quickly assess and exclude all other causes except severe bronchospasm.
- b) Briefly outline your management of this situation. (60% marks)
Answer
Answer and interpretation
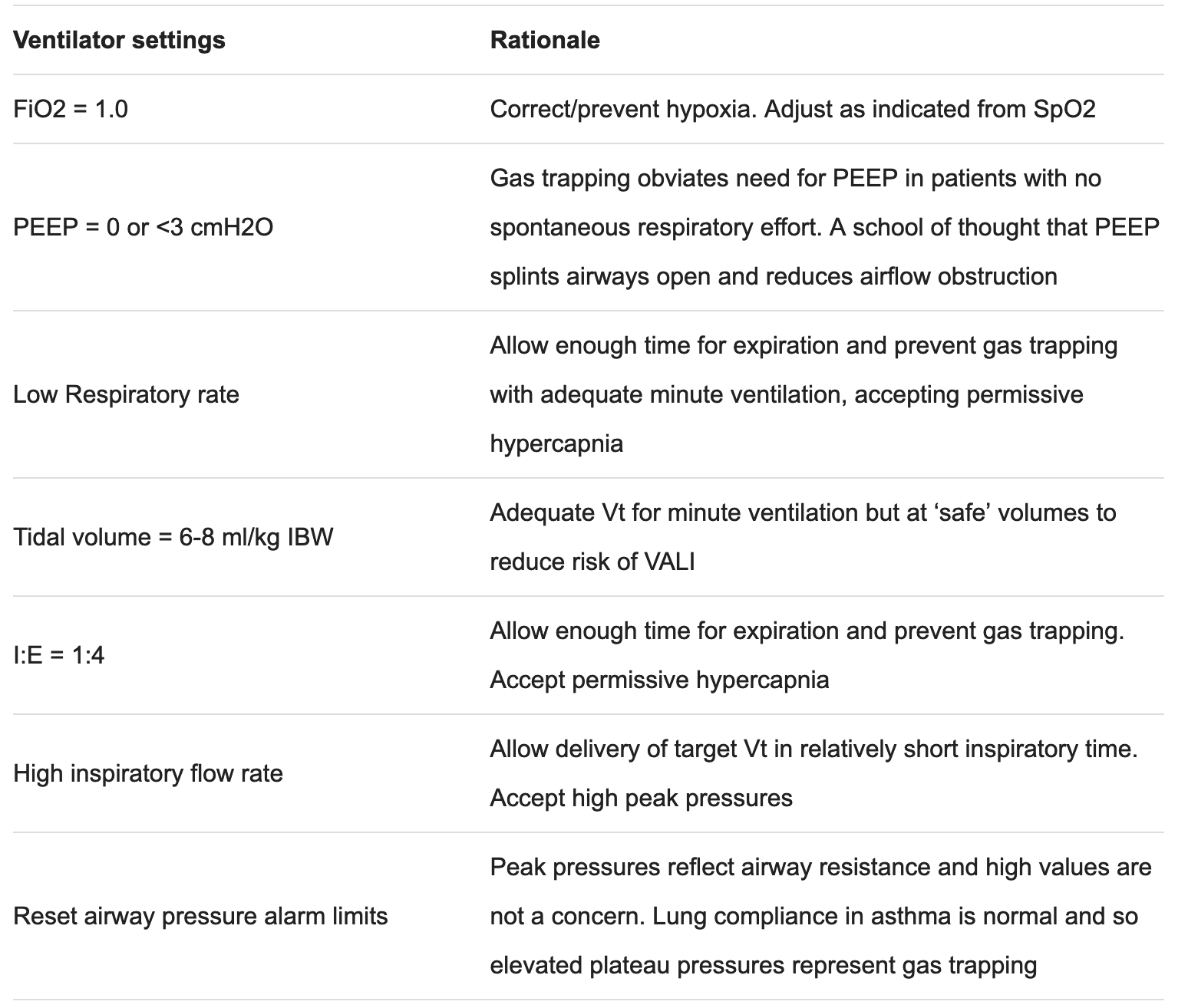
a) Describe what ventilator settings you will initially set and give the reasons for your answer. (40% marks)
b) Briefly outline your management of this situation. (60% marks)
Ensure adequate sedation:
- Ketamine +/- propofol +/- analgesia
- Preferentially use non histamine releasing analgesia – fentanyl
Muscle relaxation:
- Non steroid/non histamine releasing agents – ideally cisatracurium
Bronchodilator therapy
- Regular inhaled salbutamol – MDI, nebuliser
- IV infusion salbutamol
- IV adrenaline infusion
- Anticholinergic therapy – Ipratropium bromide inhaled regularly
- Magnesium infusion – aiming for Mg 1.5-2.5 mmol/L
- Methylxanthine therapy – Aminophylline infusion
Steroid therapy
- 100 mg 6 hrly hydrocortisone (or any reasonable steroid / dose)
Ventilation
- Confirm ventilator settings
- Tidal volume 6-8 mL/kg
- Check plateau (rather than peak) inspiratory pressure with inspiratory pause in volume control mode and paralysed patient
- Reduce respiratory rate if possible
- Minimise PEEP
- Check for evidence of dynamic hyperinflation with expiratory hold in paralysed patient
- Permissive hypercapnia
Other strategies
- Answer and interpretationInhaled volatile anaesthetic agents
- Heliox if available
- Consider ECCO2 removal / ECMO
- Pass rate: 71%
- Highest mark: 8.8
Additional comments:
- Common scenario and should be basic knowledge. Some candidates gave a poor explanation for their choice of ventilator settings in part a). Candidates who failed the question had knowledge gaps and inadequate detail in their answer.

Examination Library
CICM
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC