
![]()
CICM SAQ 2015.2 Q16
Question
You have been asked to assess a previously healthy 32-year-male who has presented following a high- speed motorbike accident. He has a Glasgow Coma Score of 15, a distended abdomen and a bleeding left leg wound. His current vital signs are as follows:
- Heart rate 120 beats/min
- Blood pressure 74/38 mmHg
- Core temp 34.7 C
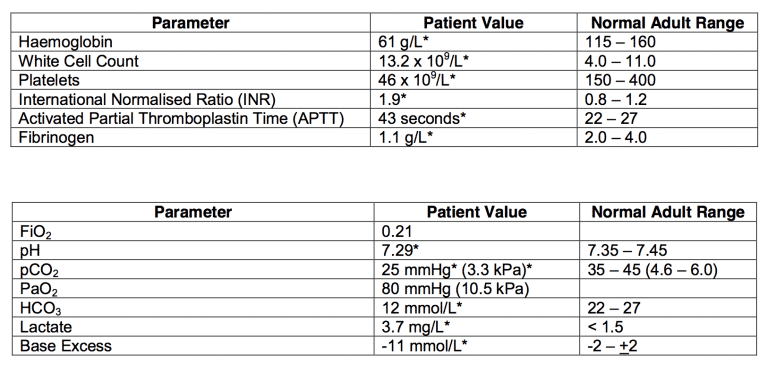
The trauma surgeon plans to perform exploratory laparotomy and open reduction and fixation of a left proximal femur fracture. The results of blood parameters and the arterial blood gas (ABG) are as follows:
- a) Describe your strategies to control the bleeding in this patient. (70% marks)
- b) What evidence is there for the use of tranexamic acid in this setting? (30% marks)
Answer
Answer and interpretation
a) Describe your strategies to control the bleeding in this patient. (70% marks)
Expedite surgery
Medical Measures to control bleeding
- Activate Massive Transfusion Protocol as per local hospital guidelines. Close liaison with surgeon
and haematologist is warranted. - Local pressure including adjunctive tourniquet use to control bleeding from the left leg wound.
- Target lower systolic blood pressure (e.g. 80 mmHg) until major bleeding has been stopped
(absence of brain injury permits the same). Permissive hypotension is tolerated and has shown
survival benefits in some studies. - Correct hypothermia and acidosis.
- Packed cells transfusion to target haemoglobin concentration 70 – 90 g/L to achieve adequate
tissue perfusion. - Fresh Frozen Plasma to maintain INR & APTT < 1.5 x mean
control. Usual dose 15 mL/kg. Cryoprecipitate to maintain Fibrinogen
levels > 1.5 g/L. Usual dose is 3-4 g or 50 mg/kg. (Fibrinogen
concentrate is also allowed). - Platelet transfusion to keep platelets > 50 x 109/L. With multiple injuries and suspicion of micro-
vascular bleeding; platelet count can be aimed at > 100 x 109/L. - Supplemental Calcium to maintain ionised calcium > 1.1 mmol/L
- Fluid Resuscitation with warmed crystalloid solutions. Aggressive fluid resuscitation is no longer
recommended due to risk of pulmonary oedema, worsening of thrombocytopenia and coagulopathy
due to haemoduilution. - Use of ROTEM/TEG targets
- Tranexamic Acid (see below)
- Recombinant Factor VIIa: Not indicated at this stage (prior to surgery)
b) What evidence is there for the use of tranexamic acid in this setting? (30% marks)
Tranexamic Acid (TXA) is a synthetic lysine analogue that is a competitive inhibitor of plasminogen. TXA is distributed throughout all tissues with plasma half-life of 120 minutes.
Evidence:
- Recently published CRASH 2 trial; a multi-centre randomised, controlled trial examined the role of TXA against placebo in trauma patients, with, or at risk of significant haemorrhage. In more than 20,000 patients; TXA demonstrated a significant reduction in all-cause mortality at 4 weeks after injury (14.5% vs. 16%; RR = 0.91, P = 0.0035) and risk of death from bleeding (4.9% vs. 5.7%; RR=0.85, p=0.00077).
- The risk of precipitated thrombosis with the use of the lysine analogues has been of major theoretical concern; however, CRASH-2 showed that the rate of thrombosis, especially myocardial infarction, was lower with the use of TXA. No adverse events were described with the use of TXA in CRASH-2, although an increased rate of seizures has been described in patients receiving a high dose of TXA when undergoing cardiac surgery.
- A further analysis of CRASH-2 data showed that early treatment (< 1 hour and 1-3 hour from injury) significantly reduced the death rate of bleeding but treatment administered after 3 hours; increased the risk of death due to bleeding. Hence, TXA should be administered within 3 hours of injury.
- TXA should be considered as adjunctive therapy in patients with traumatic haemorrhage in the setting of overall patient management; including strict attention to the control of bleeding, physiological and metabolic parameters, coagulation and temperature maintenance.
- Pass rate: 67%
- Highest mark: 7.0
Additional Examiners’ Comments:
- Most candidates answered this question well although knowledge relating to the evidence for tranexamic acid was overall limited. Some gave a reasonable discussion of the medical management of bleeding but omitted surgical strategies.

Examination Library
CICM
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC