![]()
CICM SAQ 2015.2 Q17
Question
A 45-year-old male is admitted to the Emergency Department after ingesting an unknown quantity of “headache tablets”. His initial complaints are nausea, vomiting, shortness of breath and tinnitus. Fluid resuscitation has been commenced. You are asked to assess him as he is getting more dyspnoeic.
His serum biochemistry and arterial blood gas profile are as follows:
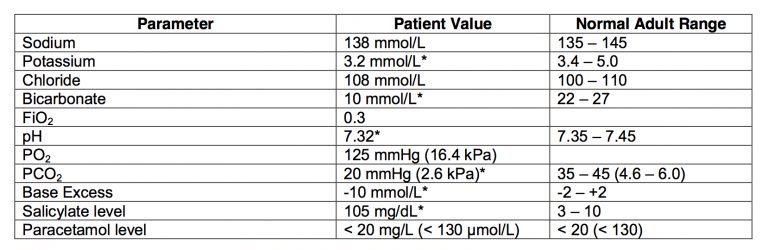
- a) Describe the acid-base status. (20% marks)
- b) What are four severe complications of this toxidrome? (20% marks)
- c) What coagulopathy may be present in this toxidrome and what is the treatment? (10% marks)
- d) What are the treatment options for severe toxicity, and what is their rationale? (50% marks)
Answer
Answer and interpretation
a) Describe the acid-base status. (20% marks)
Acid-base status:
- Increased anion gap metabolic acidosis
- Concomitant normal anion gap metabolic acidosis
- Respiratory alkalosis
- Decreased delta ratio
b) What are four severe complications of this toxidrome? (20% marks)
- Hypoglycaemia
- Pulmonary oedema
- Cerebral oedema
- Arrhythmias
- Hyperpyrexia
c) What coagulopathy may be present in this toxidrome and what is the treatment? (10% marks)
- Hypoprothrombinaemia
- Vitamin K
d) What are the treatment options for severe toxicity, and what is their rationale? (50% marks)
Forced alkaline diuresis.
- Renal excretion of salicylates becomes important when the metabolic pathways become saturated. There is a 10-20 fold increase in elimination when the urine pH increased from 5 to 8.
Haemodialysis.
- Most of the drug is protein-bound, and is concentration dependant. The volume of distribution is small, and binding site saturation leads to large levels of free drug, which is easily dialyzable.
Multiple-dose charcoal.
- Many aspirin forms are slow release and after ingestion they clump together in the GI tract, forming a large slow release preparation. It is also poorly soluble in the stomach leading to delayed absorption.
- Pass rate: 64%
- Highest mark: 9.3
Additional Examiners’ Comments:
- Most candidates understood the acid-base abnormalities but not all were able to provide cogent answers relating to the complications and management. Few were able to describe all the treatment options for severe toxicity with the rationale for these strategies.

Examination Library
CICM
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC