
![]()
CICM SAQ 2015.2 Q20
Question
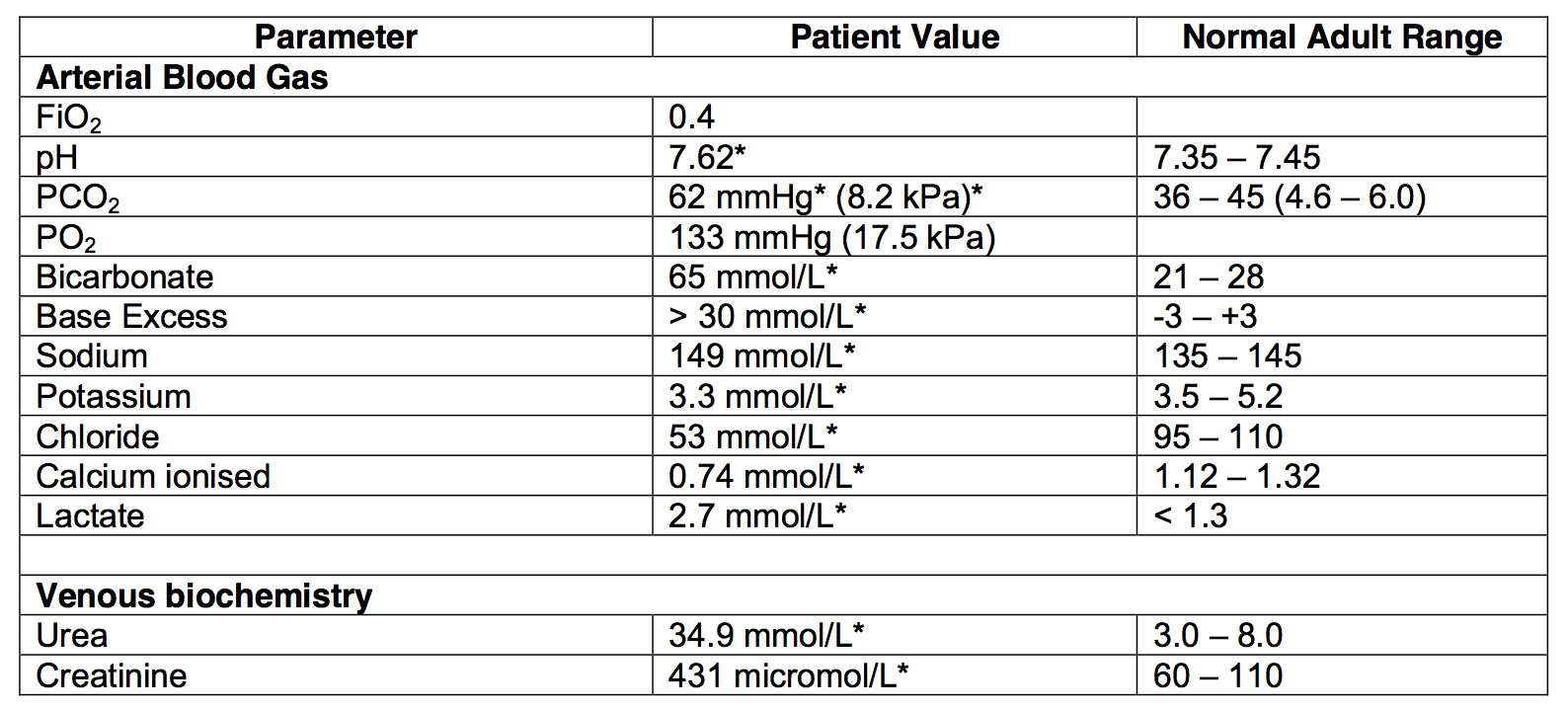
20.1 A 50-year-old male with a history of chronic pancreatitis presents with several days of nausea and vomiting. His biochemistry profile is below. Interpret the abnormalities in the above results and give likely underlying causes. (30% marks):
20.2 A 28-year-old previously fit male presents with a two-day history of fever, headache and a widespread rash. Results of investigations are below:
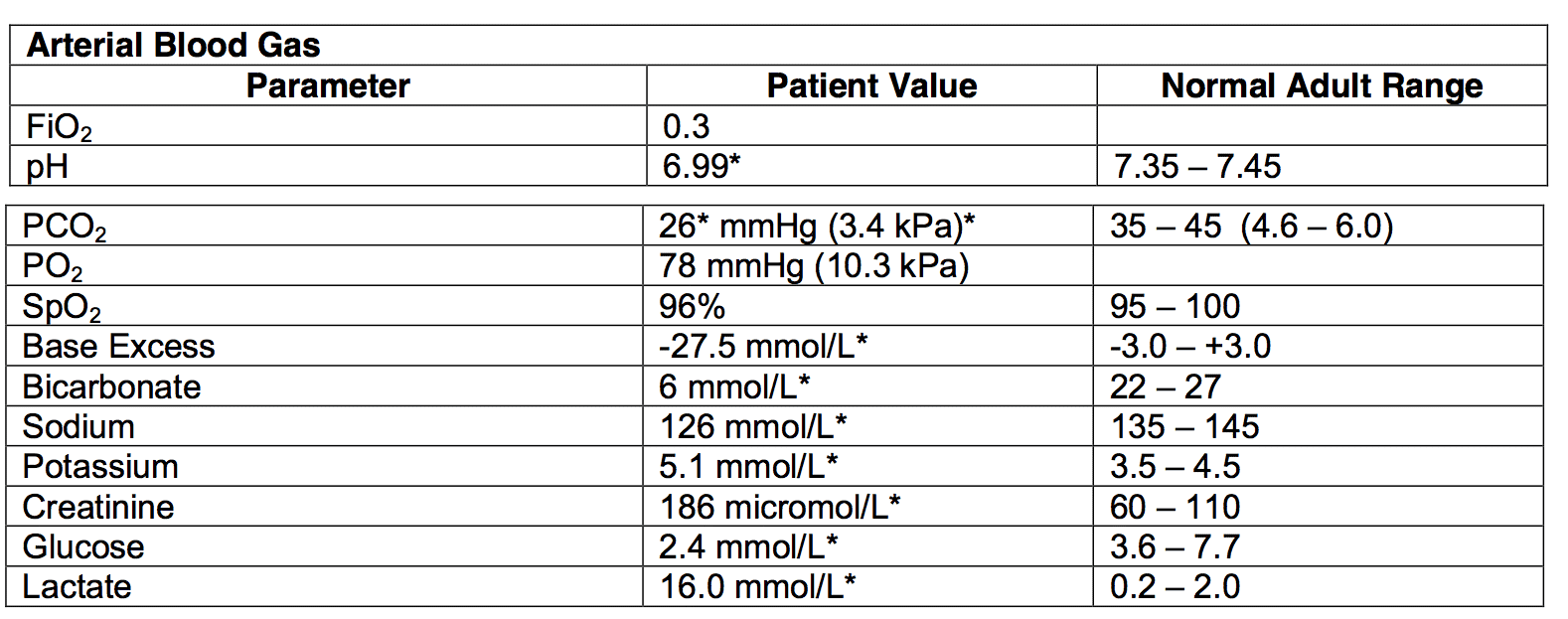
Blood cultures show Gram-negative cocci.
- a) List the abnormalities shown by the ABG. (10% marks)
- b) Give the most likely diagnosis. (5% marks)
- c) What complication of this condition may have occurred? (5% marks)
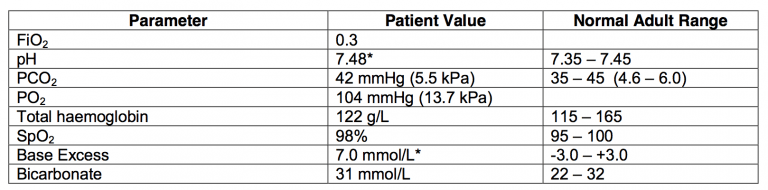
20.3 The following arterial blood gas result was obtained from a 65-year-old lady with exacerbation of chronic obstructive pulmonary disease (COPD), day 7 in ICU following intubation and ventilation for respiratory failure.
- a) Interpret the arterial blood gas. (10% marks)
- b) Give four possible reasons for the acid-base disturbance seen. (10% marks)
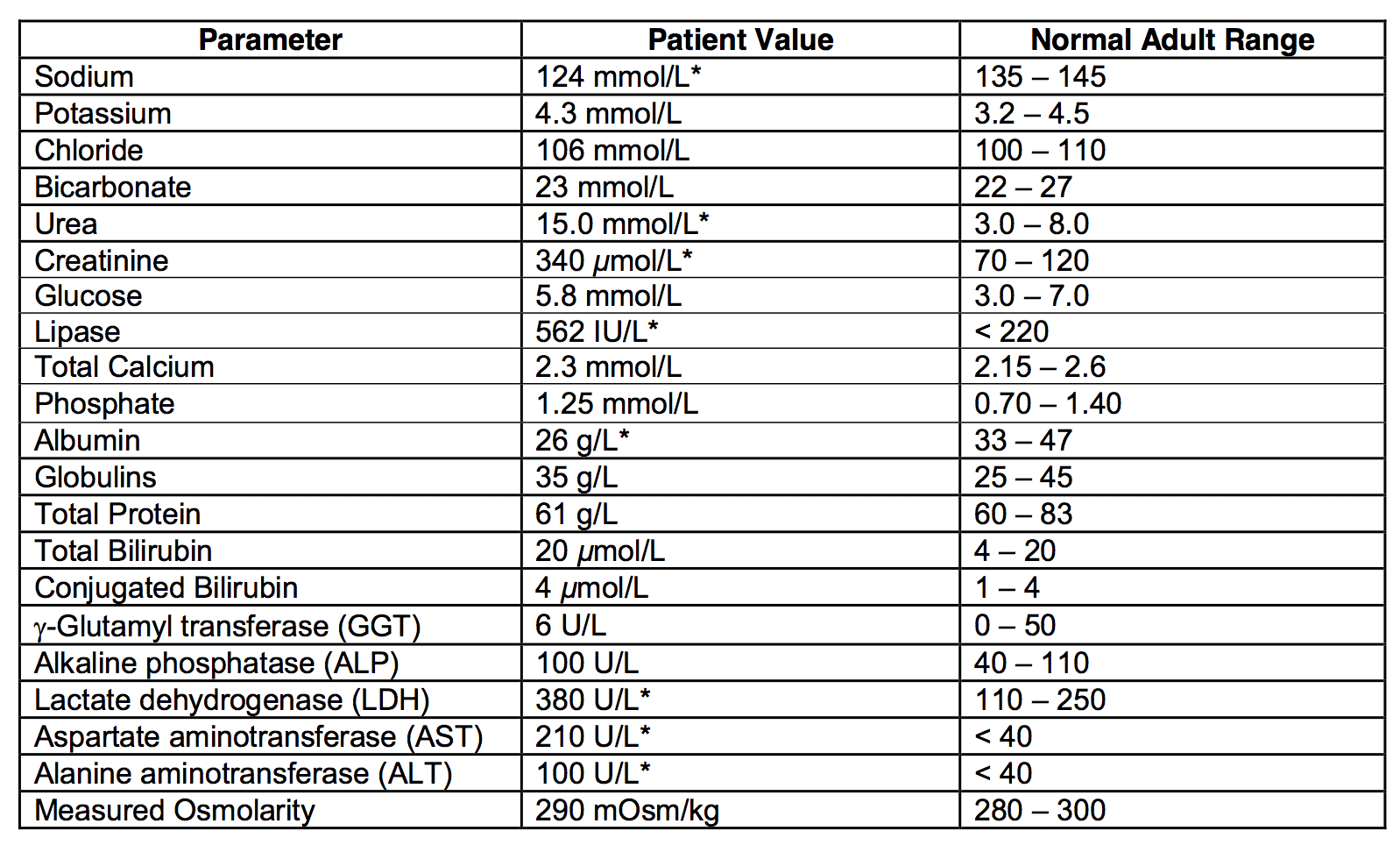
20.4 The following biochemical profile is from a 65-year-old male who has been admitted to your Intensive Care Unit with a diagnosis of pancreatitis of unknown aetiology. What blood test would you now order? Give your reasoning. (30% marks)
Answer
Answer and interpretation
20.1
- Severe metabolic alkalosis (raised SID)
- Respiratory compensation (incomplete)
- High anion gap (approx. 31) metabolic acidosis
- Profound hypochloraemia
- Gastric losses and fluid depletion causing chloride loss and metabolic alkalosis
- Metabolic acidosis secondary to renal failure (acute? Acute on chronic?) +/- sepsis from pancreatitis and/or gastro-enteritis
- CO2 retention as compensation for severe metabolic alkalosis
20.2
a) List the abnormalities shown by the ABG. (10% marks)
- Severe lactic acidosis with inadequate respiratory compensation and acute renal impairment and hypoglycaemia.
b) Give the most likely diagnosis. (5% marks)
- Meningococcal septicaemia
c) What complication of this condition may have occurred? (5% marks)
- Waterhouse-Friderichsen syndrome.
Multi-organ failure with liver and renal dysfunction is a reasonable answer and was given some credit.
20.3
a) Interpret the arterial blood gas. (10% marks)
- Metabolic alkalosis
- Raised A-a gradient
b) Give four possible reasons for the acid-base disturbance seen. (10% marks)
- Diuretics
- Steroids
- NG losses
- Post hypercapnia
20.4
- Lipid profile.
- The patient has low serum sodium but a normal measured osmolarity and hence has pseudohyponatraemia
- His glucose and protein levels are not elevated. He therefore is likely to have hypertriglyceridemia, which may be the underlying cause of his pancreatitis.
- Pass rate: 71%
- Highest mark: 8.9
Additional Examiners’ Comments:
- 20.4 was the least well answered section with many candidates failing to recognise pseudohyponatraemia.

Examination Library
CICM
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
