
![]()
CT Case 006
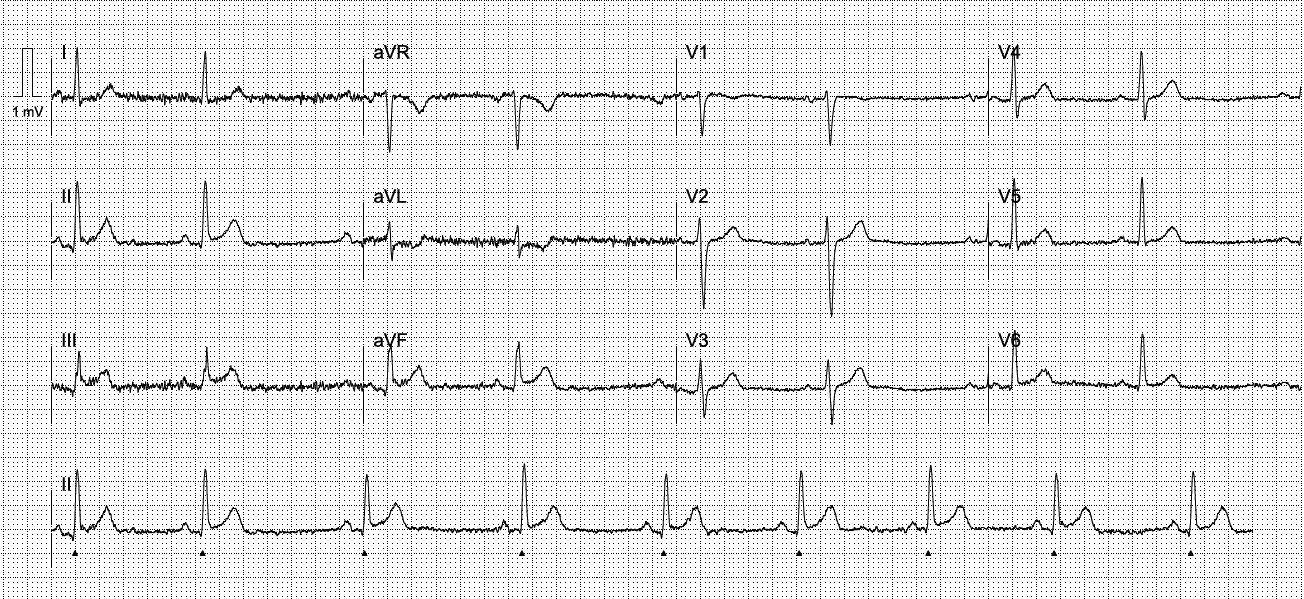
Pre-hospital cath lab activation for a 65yo male with sudden onset central crushing chest pain and some lower back pain with a STEMI pattern on ECG.
His ECG on arrival to the emergency department showed ST elevation in leads III and aVF, with a heart rate of 58
On examination he had a heart rate of 50, SBP 80 with cool peripheries. An adrenaline infusion was commenced to achieve MAP >65mmHg.
Cardiology reviewed the patient in the ED and took the patient urgently for cardiac catheterization.
Cardiac cath lab image
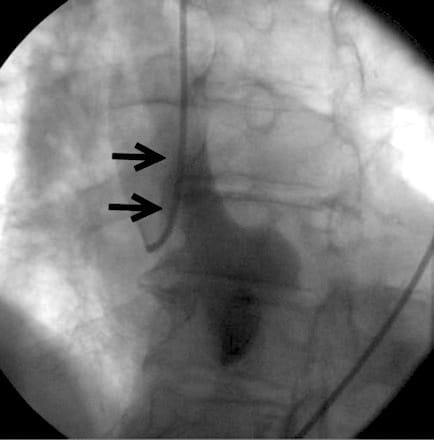
This image shows a large aortic dissection flap. Note, while this isn’t the specific image for this patient, the image demonstrates the same pathology.
In the cath lab they found that the dissection flap extended into the right coronary artery (RCA).
The patient was taken for urgent CT aortogram and then to the operating theatre.
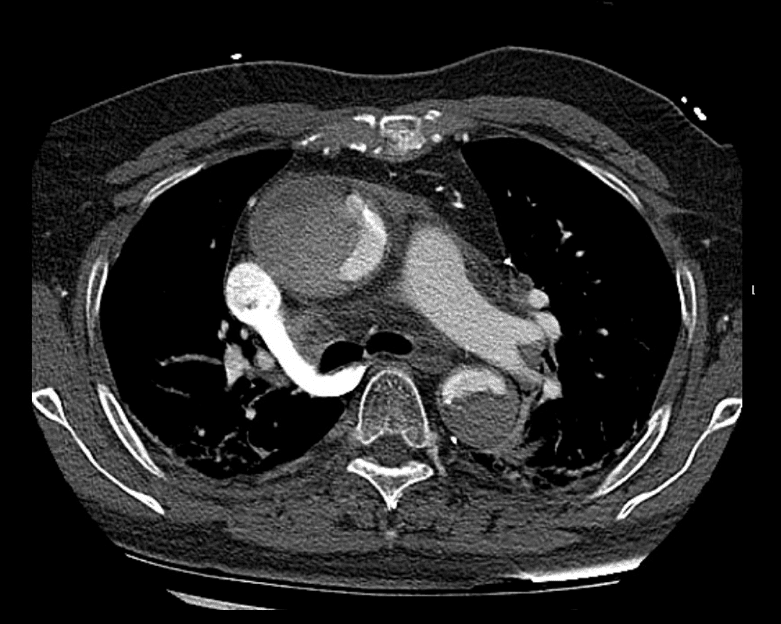
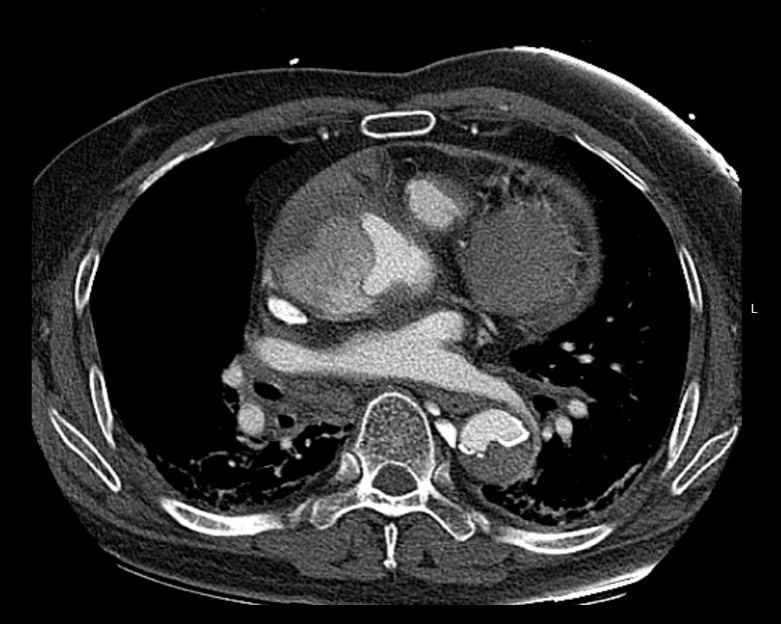
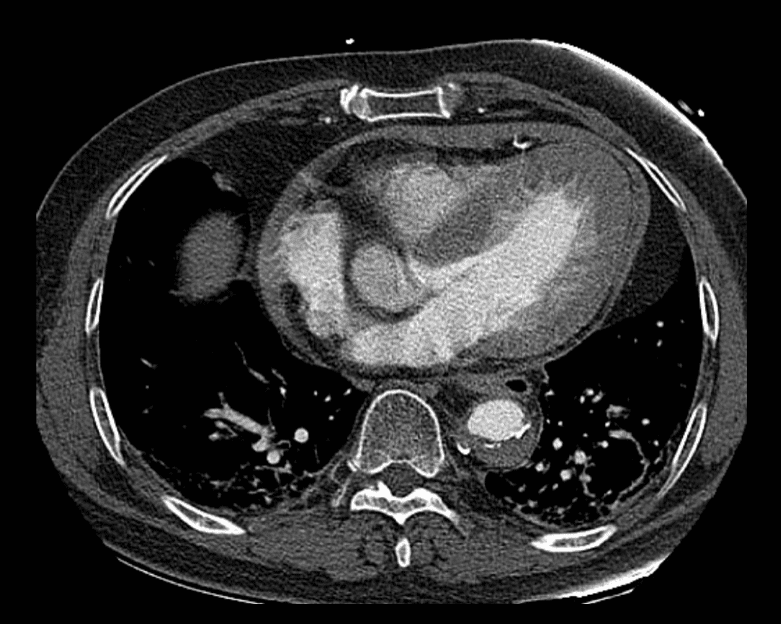
Describe and interpret the CT images
CT INTERPRETATION
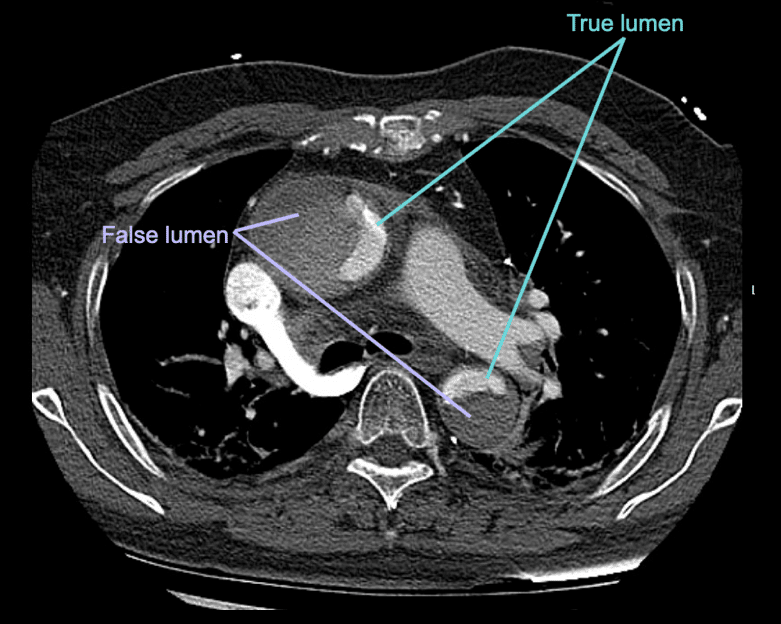
This CT shows an aortic dissection, both the ascending and the descending aorta are involved. This dissection is classified as Stanford type A as the ascending aorta is involved.
There is significant luminal narrowing with almost almost circumferential detachment of the intima.
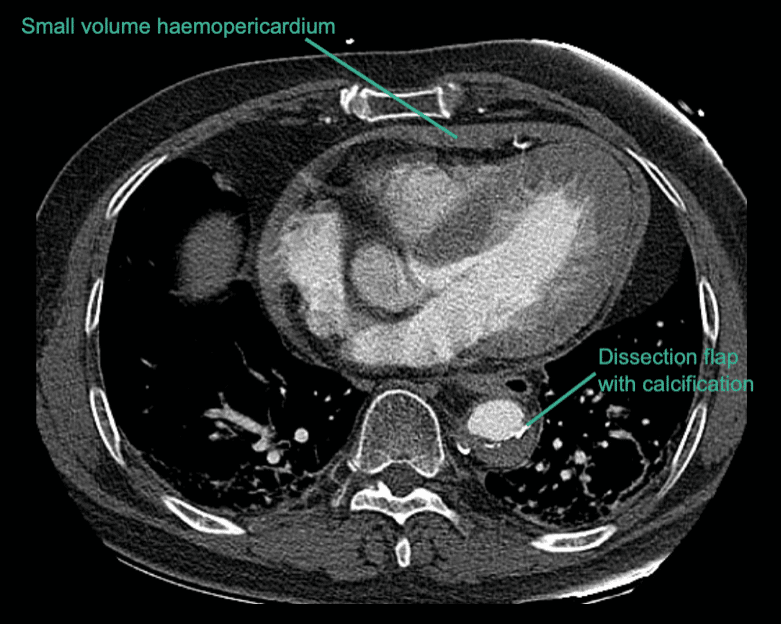
The ascending thoracic aorta is dilated to 55mm.
There is also a small haemopericardium.

CLINICAL CORRELATION
Aortic dissection is one of the great STEMI mimics. It must always be considered, especially when there is a history of concurrent chest AND back pain.
ST elevation in III and aVF is the typical pattern seen when aortic dissection causes coronary artery occlusion. This is because a dissection more commonly originates from the right anterior aspect of the ascending aorta (near the origin of the RCA).
The mechanism of infarction can be either extension of the dissection into the coronary artery, or occlusion of the coronary ostia from the dissection flap. See the great image below demonstrating this:

This is just one of the many possible complications of aortic dissection. Other complications to assess for in aortic dissection include:
- Rupture into body cavity – intra-abdominal, haemothorax, haemopericardium
- Occlusion of branches – causing stroke, spinal cord ischaemia, limb ischaemia, myocardial ischaemic
- Aortic regurgitation due to disruption of the aortic root structure
REFERENCES
- Cai J, Cao Y, Yuan H, Yang K, Zhu YS. Inferior myocardial infarction secondary to aortic dissection associated with bicuspid aortic valve. J Cardiovasc Dis Res. 2012 Apr;3(2):138-42.
- Chen A, Ren X. Aortic Dissection Manifesting as ST-Segment-Elevation Myocardial Infarction. Circulation. 2015 May 26;131(21):e503-4
[cite]
TOP 100 CT SERIES

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney