![]()
CT Case 013
A 65yo man presents with progressive drowsiness and confusion with a 1-week duration of dull headache.
His past medical history includes end stage renal failure, Type II diabetes and hypertension.
Describe and interpret the CT images
CT Head INTERPRETATION
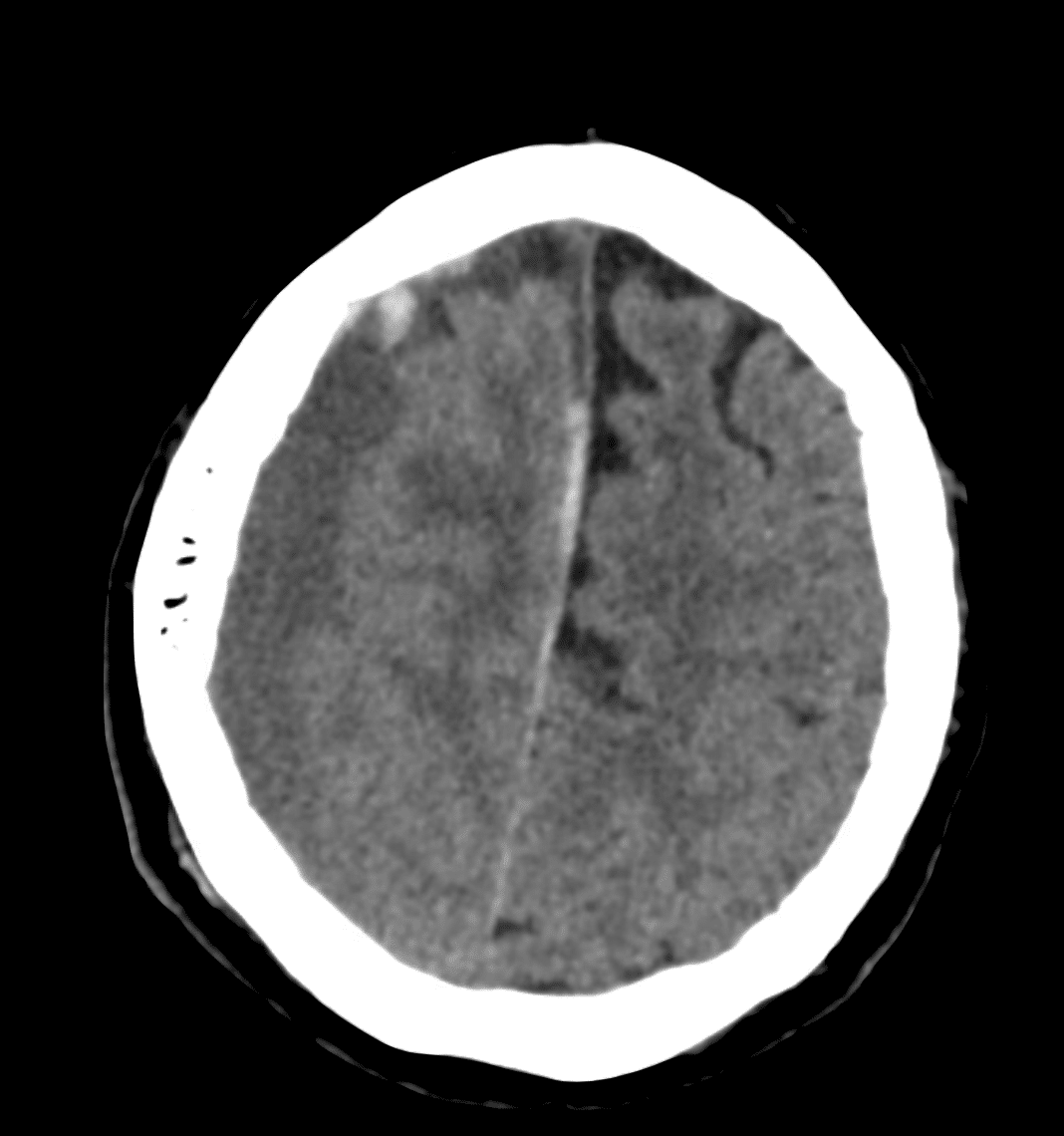
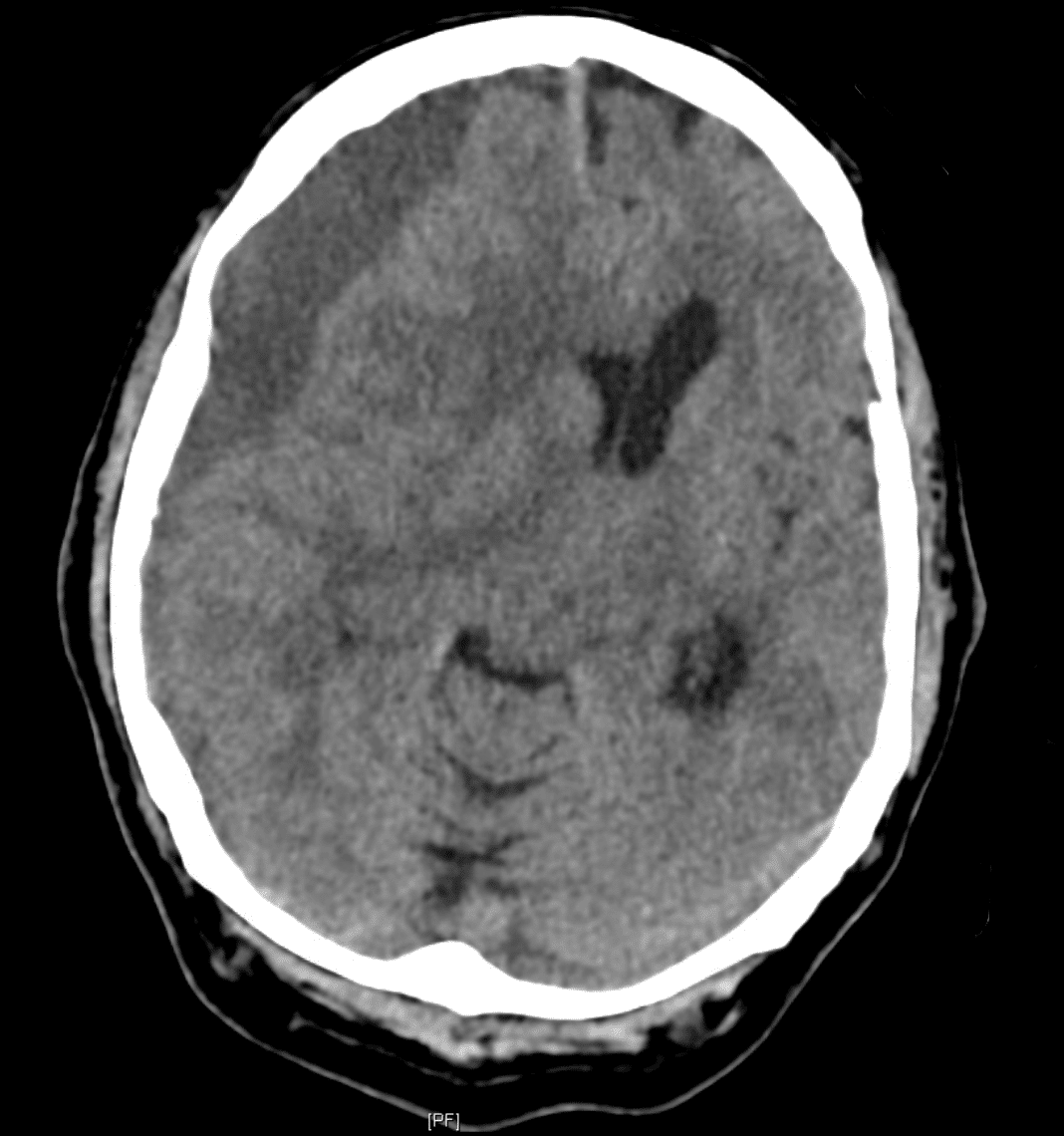
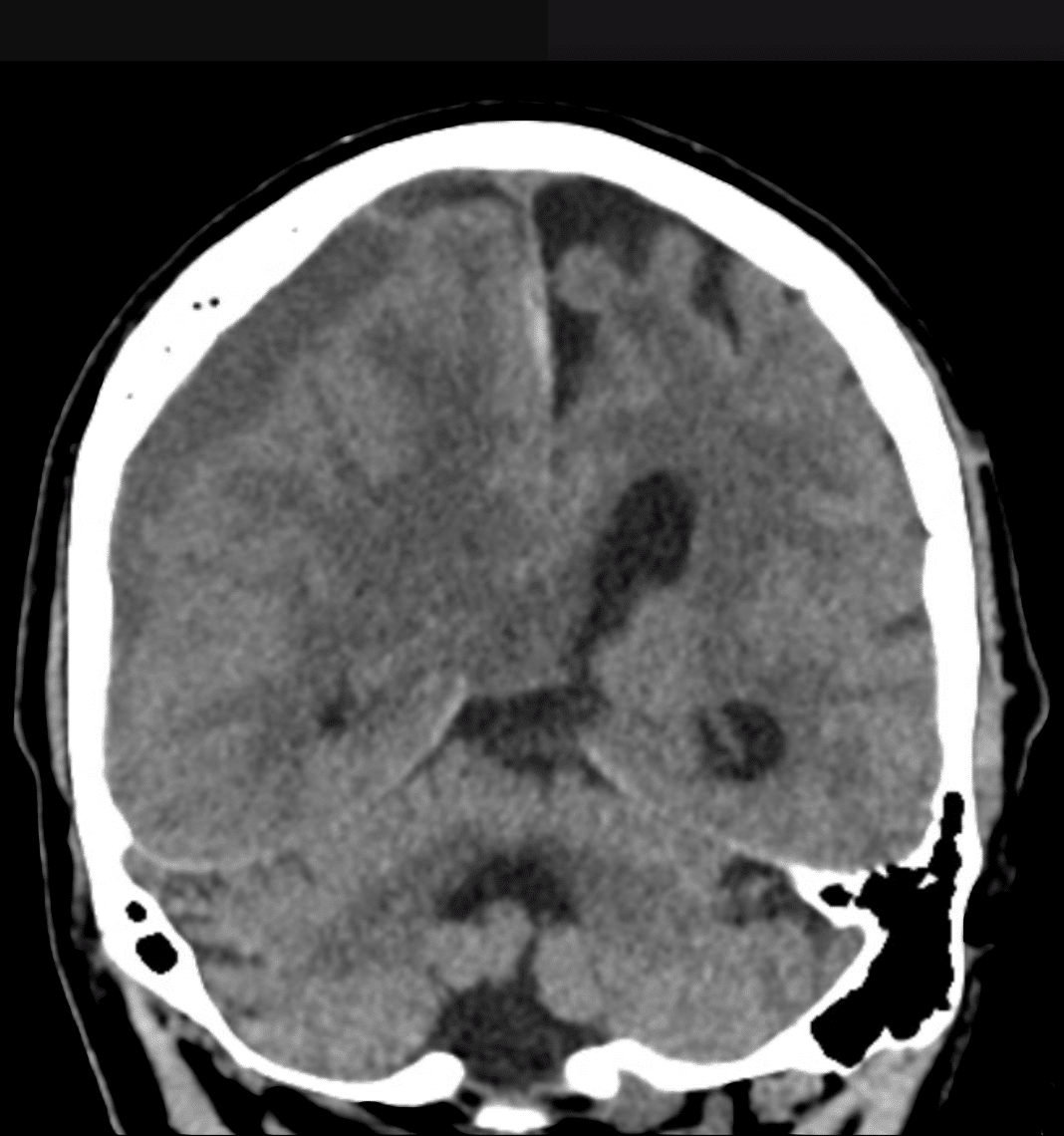
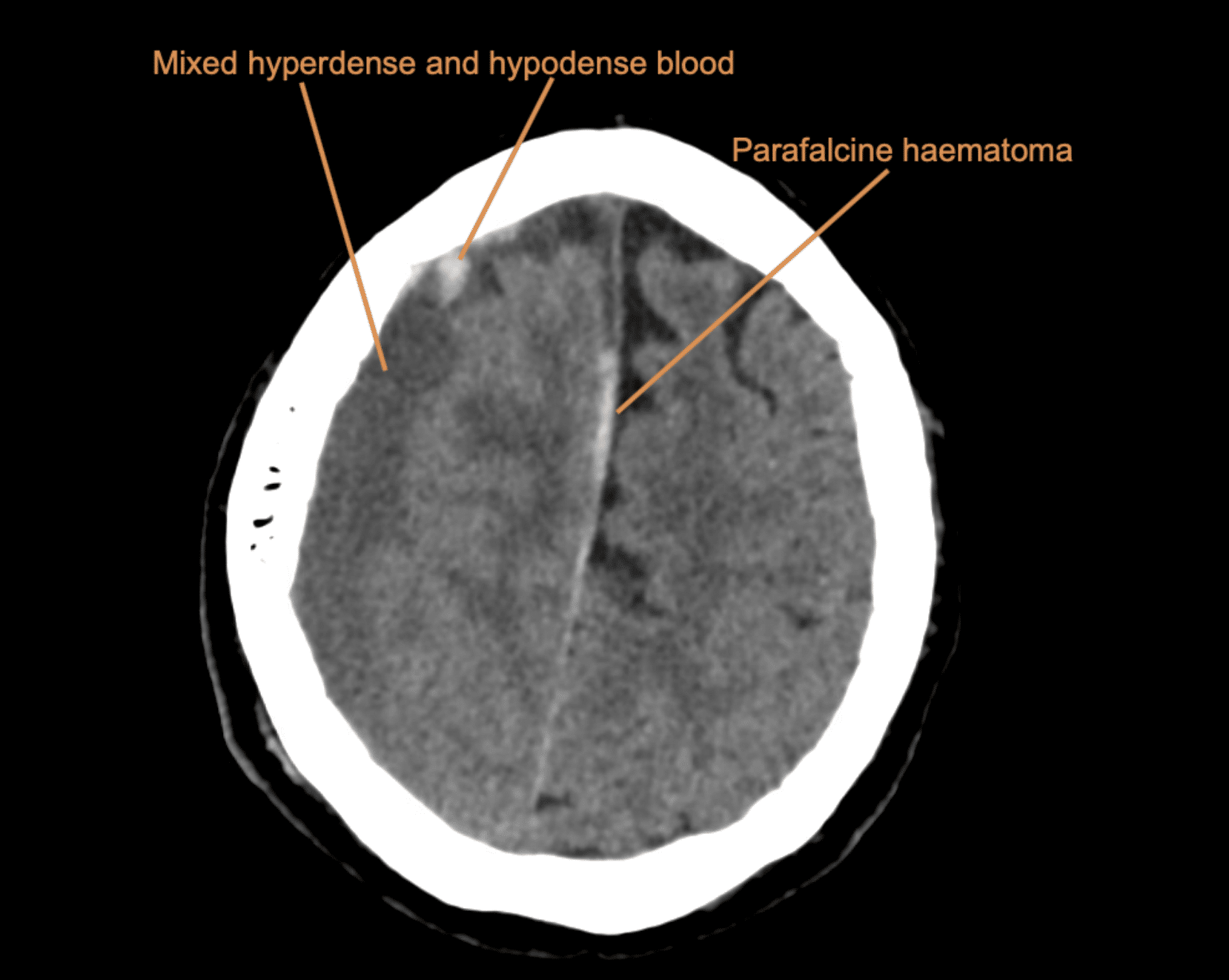
There is a large right sided subdural haematoma (maximum thickness of 23mm).
Mostly it is hypodense. However, there is an area of hyperdense blood in the frontal region.
There is also a parafalcine subdural haemorrhage extending along the right side of the falx cerebri.
There are signs of mass effect (other structures are being displaced due to the real estate that the haematoma is taking up within the finite cranial cavity). Signs include:
- 23mm of midline shift to the left
- Right subflacine herniation and early right uncal herniation
- Almost complete effacement of the right lateral ventricle with prominence of the temporal horn (suggesting hydrocephalus)


CLINICAL CORRELATION
When we talk about extra-axial bleeds (these are bleeds what are within the skull but outside of the brain tissue) there are three types with distinct patterns:

This case has a typical appearance of subdural haemorrhage. The blood wraps around the brain in a crescent shape. And, unlike extradural haemorrhage it is able to cross the suture lines.
The mixed density of the blood here tells us that this is an acute on chronic bleed.
Acute fresh blood being higher in density, and chronic blood being lower in density as the clot starts to degrade.
Density can be measured using Hounsfield units, but we can also make an estimate of density by comparing the blood density to the density of brain tissue;
- Acute – more-dense than the brain tissue
- Subacute – same density as brain tissue
- Chronic – less dense than brain tissue
Note: Hyperacute (< 2hrs) blood hasn’t had a chance to clot yet, this will also look less dense than brain tissue.
This case also demonstrates a parafalcine subdural haemorrhage, meaning a subdural haemorrhage running just next to the falx cerebri. When it occurs in isolation it is one of the most commonly missed types of intracranial haemorrhage. It can be easily missed because the blood gets misinterpreted as being the dural fold of the falx cerebri.
Outcome
This patient went on to have urgent decompression of this large subdural haemorrhage.
Repeat CT showed resolution of the midline shift and he had a good clinical improvement.
REFERENCES
- Beech G. CT Case 002. LITFL
[cite]
TOP 100 CT SERIES

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney