
![]()
CT Case 026
A 21yo female is brought in by ambulance. She was the driver of a vehicle involved in a head on crash at 70kph.
On arrival BP 90/56, HR 120, GCS 15. Complaining of generalised abdominal pain with peritonism. Seatbelt abrasion over lower abdomen.
EFAST shows free fluid in RUQ, LUQ and pelvis. The patient was taken for an urgent CT scan
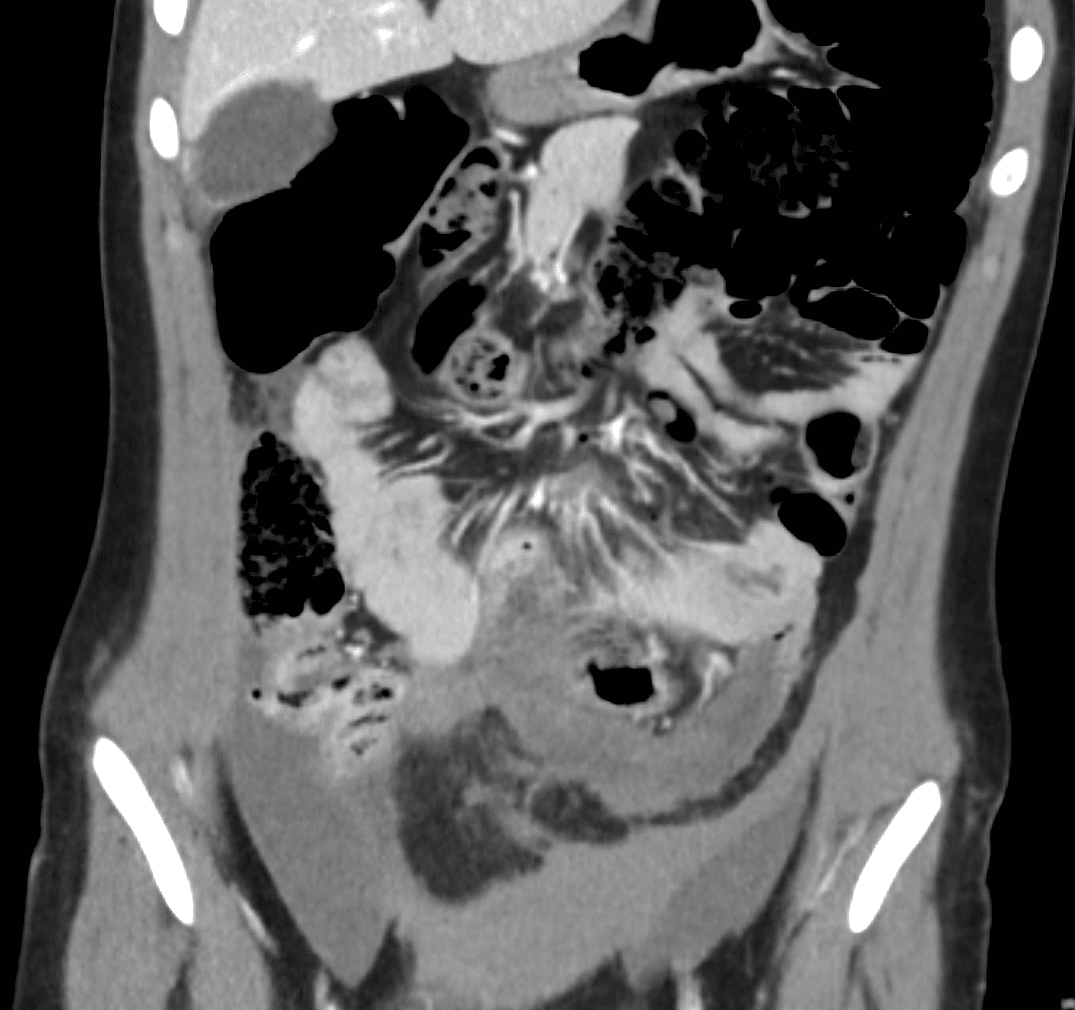



Describe and interpret the CT images
CT INTERPRETATION
There is a long segment (15cm) of proximal jejunal bowel wall thickening with nonenhancement. This is consistent with bowel infarction. In trauma, this is usually due to a mesenteric tear causing de-vascularisation of a segment of bowel (see case 27 for more discussion of features of bowel infarct).
There is pneumoperitoneum and moderate volume free intra-peritoneal fluid.
There is also a small laceration through the inferior pole of the spleen. This is consistent with a grade 1 splenic laceration.
There is transverse subcutaneous fat stranding across the lower abdomen, in keeping the seatbelt sign.




CLINICAL CORRELATION
These CT features are compatible with traumatic mesenteric tear and infarction of the jejunum with associated perforation. In blunt trauma, pneumoperitoneum indicates hollow viscus perforation.
Hyperdense free fluid indicates haemoperitoneum.

Jejunal devascularisation is a classical injury pattern seen in restrained passengers of a high speed MVA. A deceleration injury occurs when the stabilised portion of the organ (the posterior abdominal wall) ceases to move forward while the mobile portion (the jejunum) continues to move forward. This results in shearing injury to the mesentery.
This patient went for urgent laparoscopy, which was subsequently converted to laparotomy due to more extensive injuries identified intra-operatively.

In addition to the jejunal injury seen on CT, in theatre she was found to have several omental bucket handle injuries causing devascularisation of the right hemicolon.
As with the described jejunal injury, a bucket handle injury is a result of sheering forces. It causes complete separation of the intestine from the mesentery, leaving a devascularised segment of bowel that looks like a handle of a bucket.
The patient required right hemicolectomy as well as resection of two segments of jejunum.
In this case we see that the intra-operative injuries are far more extensive than the injuries seen on CT scan. Due to the insensitivity of CT for identifying traumatic bowel injury, it has consistently been found to be the most common traumatic abdominopelvic injury to be missed on CT.
References
- Hartung MP. Abdomen CT: Trauma. Medmastery
- Demetriades D, Inaba, K. Abdominal Injury. In Demetriades D & Newton E. (Authors), Color Atlas of Emergency Trauma. 2018: 119-159. Cambridge: Cambridge University Press.
- Altadill AR. Bowel and mesenteric trauma. Radiopaedia
[cite]
TOP 100 CT SERIES

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Provisional fellow in emergency radiology, Liverpool hospital, Sydney. Other areas of interest include paediatric and cardiac imaging.

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.
