
![]()
CT Case 038
A 60-year-old man presents with chronic cough, worse in the last 2 weeks with new hoarse voice and new left upper limb swelling. He also has mild pleuritic left sided chest pain.
On examination
- Frequent dry cough with reduced air entry to the entire left hemithorax.
- Distended neck veins on the left side with mild oedema to the face and pitting oedema to left arm.
- Enlarged non-tender left cervical lymph nodes
- Pemberton manouver associated with facial plethora, cyanosis and distension of neck veins (Pemberton sign +ve)
A Chest X-Ray is taken on arrival
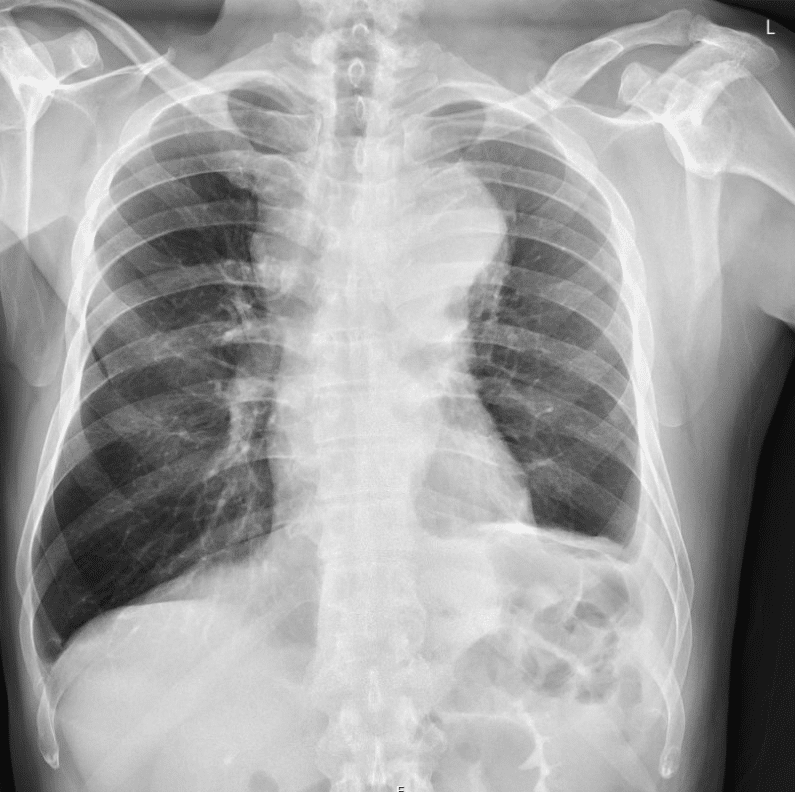
Describe and interpret the CXR
CXR INTERPRETATION
There is a widened appearance of the mediastinal contour.
The left lung shows volume loss compared to the right (note the raised left hemidiaphragm).
There is blunting of left costophrenic angle with lateral upward sloping which is a sign of an effusion.
The mediastinal widening raises suspicious for enlarged mediastinal LNs or mass.

The patient went on to have a CT of his neck and chest


Describe and interpret the CT images
CT INTERPRETATION
There is extensive pathological confluent lymphadenopathy in the lower neck and mediastinum with associated thrombosis of the right brachiocephalic vein and a short segment thrombosis of the SVC. The centre of the confluent lymph nodes is less dense which suggests central necrosis.
Differential considerations include a proximal bronchogenic carcinoma, lymphoproliferative disorder or a hypopharyngeal carcinoma


CLINICAL CORRELATION
Superior Vena Cava Obstruction
This case demonstrates thrombus of the brachiocephalic vein and SVC in the context of malignancy.
A number of causes of SVC obstruction exist, in this case it is a combination of SVC thrombus as well as extensive mediastinal lymphadenopathy secondary to malignancy.
The malignancy was found to be a poorly differentiated adenocarcinoma, it was unclear if the origin was head and neck or lung. This patient was admitted for therapeutic anticoagulation as well as targeted radiotherapy. He also went on to have a SVC stent inserted for progressive SVC occlusion
Key signs of SVC obstruction on examination include:
- oedema to face, neck, upper torso, upper limbs
- cough, dyspnea
- hoarse voice
- Pemberton sign – facial plethora, cyanosis and distended neck veins when both arms are raised simultaneously
- venous collaterals on the chest
References
- Cadogan M. Pemberton Sign. LITFL
TOP 100 CT SERIES

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Provisional fellow in emergency radiology, Liverpool hospital, Sydney. Other areas of interest include paediatric and cardiac imaging.

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.

Love the case, so relevant to board exams, I wish you also covered differentials like pancoast tumours or leukostasis. Anyways it’s great.