![]()
CT Case 040
A 26-year-old male is brought in by ambulance with vision loss since this morning. He describes 2 weeks of dull headache, with intermittent blurred vision. He has no significant past medical history
He presents with worsening symptoms – almost complete loss of vision bilaterally (only able to discern lights), and progressive headache.
On examination he is tachycardiac (125bpm) and hypertensive (210/170)
Aside from loss of vision, he has no other neurological deficit.
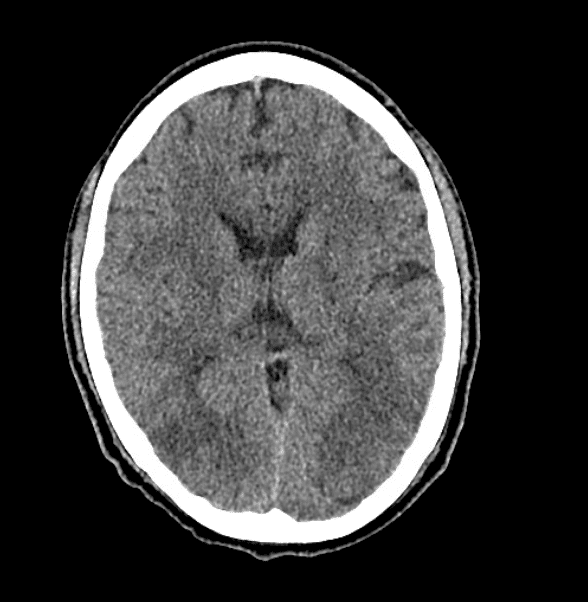



Describe and interpret the CT scan
CT INTERPRETATION
There is vasogenic white matter oedema in the occipital region (note the increase in contrast between the grey and the white matter).
There is abnormal perfusion in the bilateral occipital lobes, with a marked raise in TMax.
TMax is the time delay between the contrast bolus arriving in the proximal large vessel arterial circulation and the brain parenchyma.
Raised TMax can also be seen I infarction. However, by looking at the CBV (cerebral blood volume) and CBF (cerebral blood flow) maps which are normal, we know this is not due to infarction.
(note the colour scale on the left-hand side of each image).
Normal values are listed below
Gray matter
- TMax: 4 s
- CBF: 60 mL/100 g/min
- CBV: 4 mL/100 g
White matter
- TMax: 4.8 s
- CBF: 25 mL/100 g/min
- CBV: 2 mL/100 g
These CT findings (of posterior circulation oedema, and delayed flow to the posterior circulation) along with the clinical picture of severe hypertension and vision loss are highly suggested of Posterior Reversible Encephalopathy Syndrome (PRES).


CLINICAL CORRELATION
Posterior Reversible Encephalopathy Syndrome (PRES)
PRES is a rare neurological emergency. It occurs when the posterior circulation of the brain is unable to autoregulate in response to an acute increase in blood pressure.
This results in disruption of the blood-brain barrier with resultant vasogenicoedema.
The parieto-occipital regions are most affected, however despite the name, any part of the brain can be involved. Cortical and sub-cortical regions could be involved, though commonly a predominant subcortical white matter involvement is seen.
Though termed as ‘reversible’, the imaging findings can show persistent/ permanent changes in some cases.
MRI is the confirmatory investigation for PRES. However, the combination of clinical findings and CT scans are enough to identify the diagnosis and commence treatment.
Other clinical findings sometimes seen in PRES are altered mental state and seizures.
The clinical priority is to promptly lower the blood pressure in order to prevent irreversible neurological damage.
It is also important to look for signs of other end organ damage secondary to the severe hypertension (such as cardiac, hepatic, renal and ophthalmic).
It is vital of course to identify and treat the precipitating cause of hypertension. In this case, the marked tachycardiac along with the hypertension made phaeochromocytoma a possible diagnosis.
In phaeochromocytoma, high circulating catecholamine levels stimulates alpha receptors.
There is a risk of unopposed alpha receptor-mediated vasoconstriction when a beta blocker is administered in a patient without adequate alpha blockade. This can precipitate or worsen a hypertensive crisis.
This patient’s blood pressure was therefore managed first with alpha blockade (Prazosin) and then only after alpha blockade was established, a high dose Labetalol infusion commenced.
Labetalol was the preferred beta blocker in this case, due to its action in blocking both alpha and beta receptors.
References
- Nickson C. PRES. LITFL
- Wiesbauer F. Hypertension. Medmastery
- Radiopaedia — Posterior Reversible Encephalopathy Syndrome (PRES)
TOP 100 CT SERIES

Provisional fellow in emergency radiology, Liverpool hospital, Sydney. Other areas of interest include paediatric and cardiac imaging.

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).