![]()
CT Case 095
A 70-year-old woman presented to the ED two weeks following a COVID infection.
She presents due to right sided neck pain, difficulty swallowing and limited mouth opening.
A CT neck series is performed

Describe and interpret the CT scans
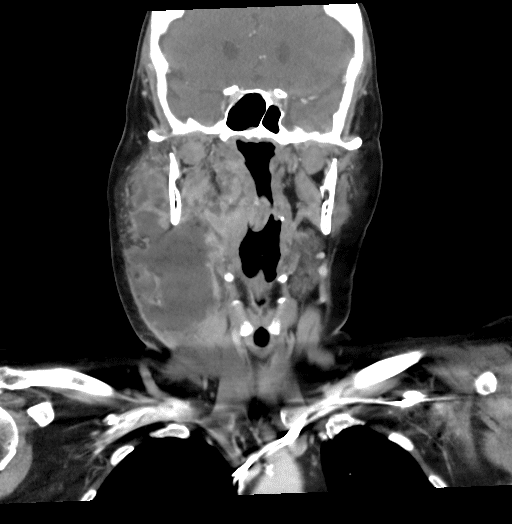
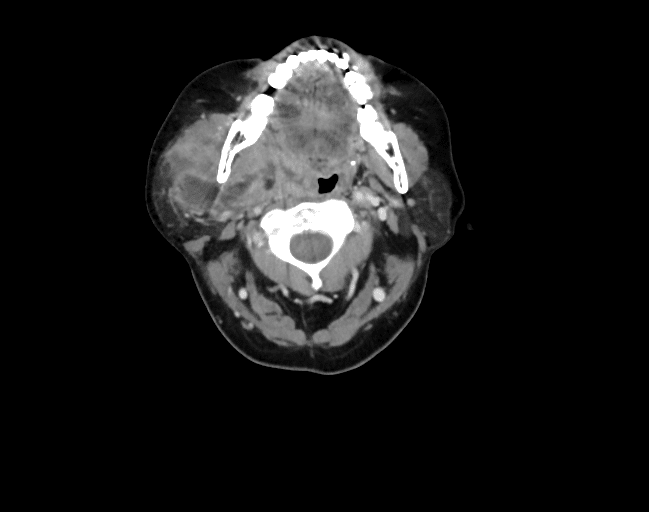
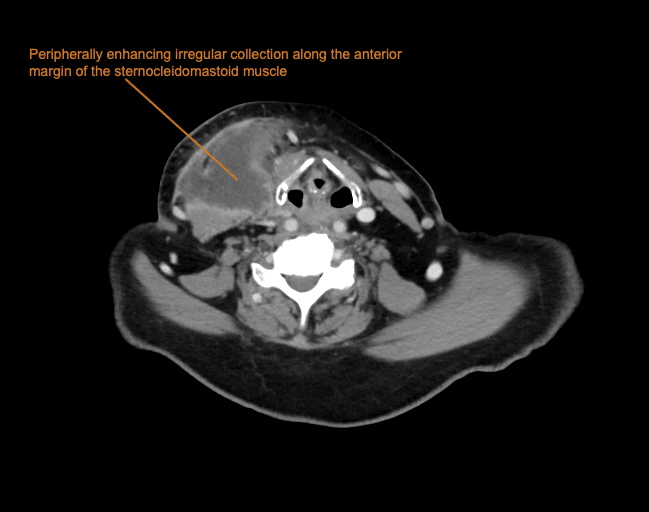
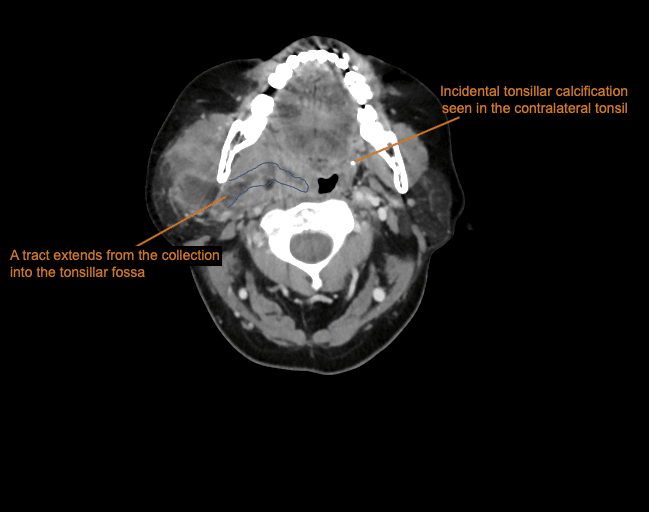
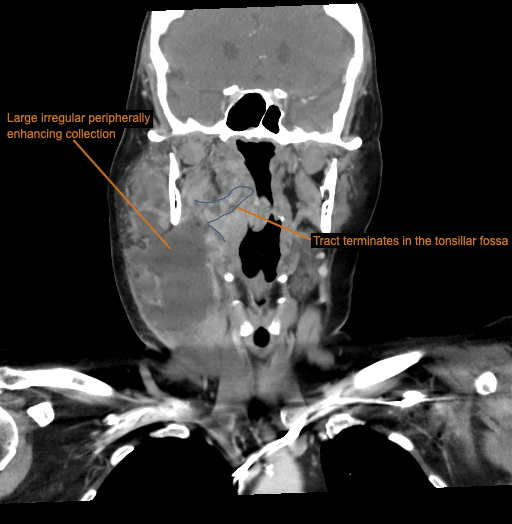
There is a large peripherally enhancing irregular collection along anterior margin of sternocleidomastoid muscle with adjacent fat stranding.
The collection extends superiorly involving multiple neck spaces including masticator space, parotid space and submandibular space due to its large size.
A tract is seen extending from the collection into the tonsillar fossa (tonsillar calcification is seen in the contralateral tonsil).
The location of the collection along the anterior margin of sternocleidomastoid and termination in a tract in the tonsillar fossa is highly suggestive of a branchial cyst.
A simple branchial cyst does not show thick peripheral enhancement and inflammatory changes, these features are only seen here as the branchial cleft cyst has become infected.
Clinical Pearls
This patient was managed with intravenous antibiotics and she was taken to theatre for incision and drainage.
Branchial cleft cysts are congenital epithelial cysts, which result from elements of the ‘branchial (pharyngeal) apparatus’ becoming entrapped during embryogenesis.
They are benign lesions. Typically, they are first identified in childhood. They appear as a non-tender fluctuant mass along the anterior border of the sternocleidomastoid muscle.
Often, they are first identified when a previously unrecognised cyst becomes infected, causing pain and increased swelling. This typically occurs after an upper respiratory tract infection.
Only a very small percentage will first present in adulthood.
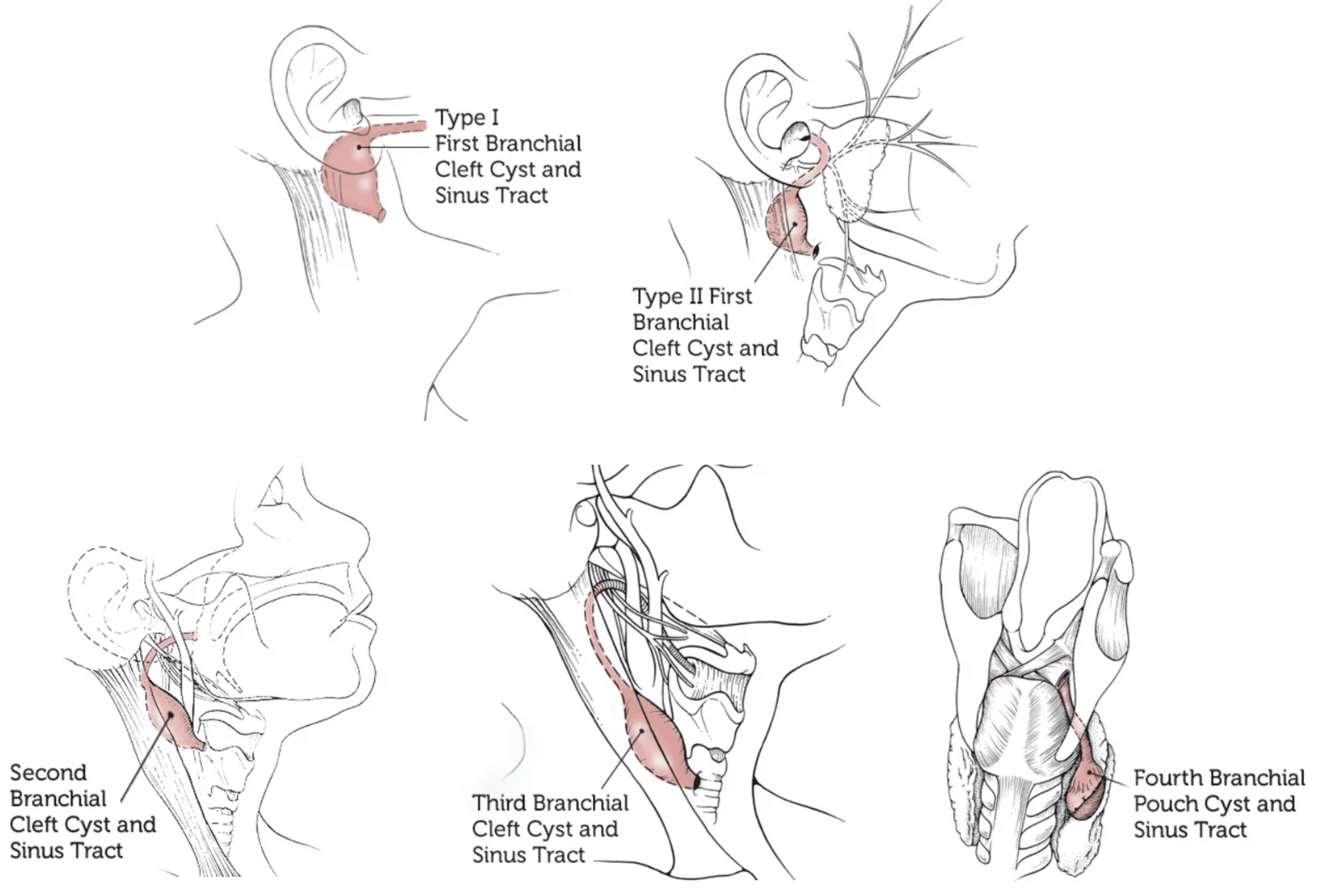
Branchial cleft cysts are subdivided based on the developmental origin and given the names first, second and third branchial cleft cysts.
Of the subtypes, second branchial cleft cysts (seen in this case) are the most common.
Second branchial cleft cysts are located just inferior to the angle of the mandible and anterior to the sternocleidomastoid muscle. The sinus tract of a second branchial cleft cyst travels through the deep structures of the neck and opens into the tonsillar fossa.
Recurrent infections of branchial cysts do occur, and fistula tracts to the skin may develop.
Once the infection has resolved, the mass is usually excised in a subsequent surgical procedure to prevent recurrent infections.
References
- Branchial Cleft Cyst. Boston Children’s Hospital
- Kumar R, Sikka K, Sagar P, Kakkar A, Thakar A. First branchial cleft anomalies: avoiding the misdiagnosis. Indian J Otolaryngol Head Neck Surg. 2013 Jul;65(3):260-3.
TOP 100 CT SERIES

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Provisional fellow in emergency radiology, Liverpool hospital, Sydney. Other areas of interest include paediatric and cardiac imaging.