
![]()
CT Case 096
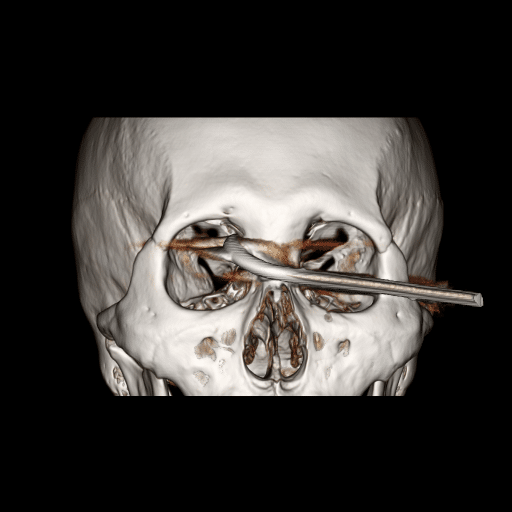
30-year-old male presents following a work place injury. A 20cm metal rod has fallen on his face, resulting in a penetrating orbital injury.
On examination there is a metal rod penetrating his right orbit medially. Despite this, his visual acuity is 6/12 bilaterally. His intraocular pressures are 15mmHg and there is no relative afferent pupillary defect (RAPD). He is GCS 15
CT brain and orbits is performed


Describe and interpret the CT scans
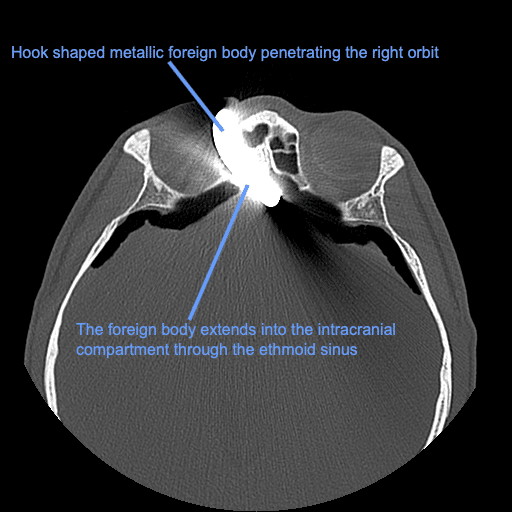
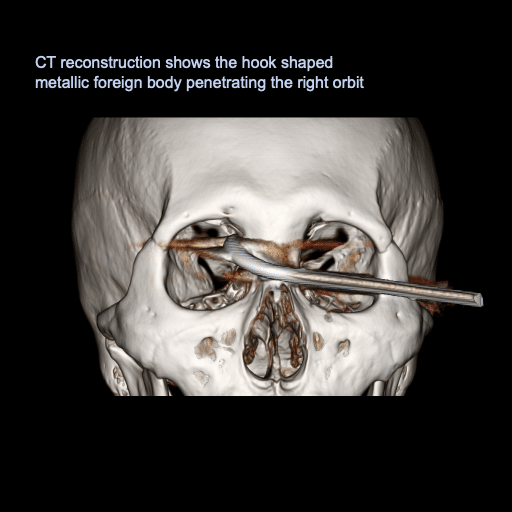
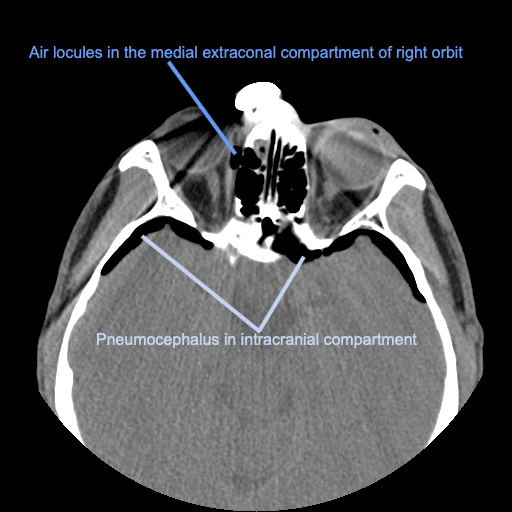
There is a hook shaped metallic foreign body penetrating the right orbit and extending into the intracranial compartment through the ethmoid sinus.
There are air locules in medial extraconal compartment of the right orbit. The globe itself appears intact.
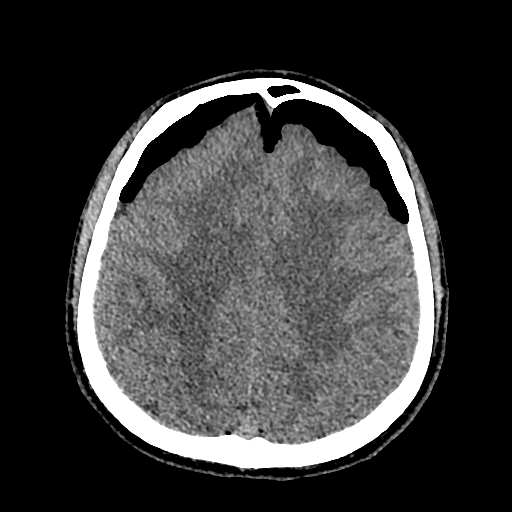
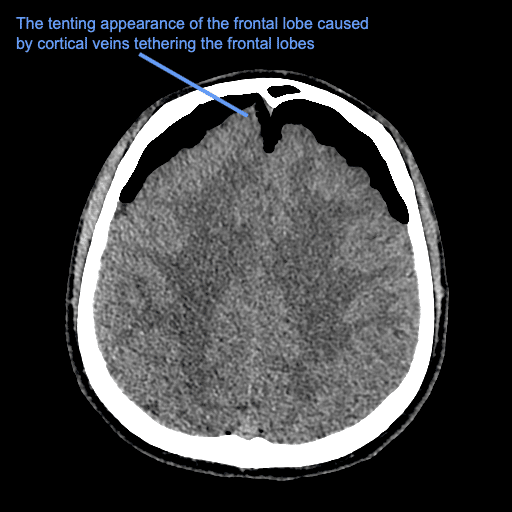
There is extensive extra-axial pneumocephalus in the bilateral frontal regions with a heaped-up appearance of the frontal lobes with widening of the inter-hemispheric space between the frontal lobes, indicating tension pneumocephalus. This appearance is known as the Mount Fuji sign and suggests that the pressure of the gas is at least greater than the surface tension of the CSF between the frontal lobes.
The tenting appearance of the right frontal lobe is caused by cortical veins tethering the frontal lobes.
Clinical Pearls
Penetrating injuries affecting the skull base are uncommon, compromising only 0.4% of head injuries.
Principles of management are removal of foreign body, prevention of infection, management of vascular injuries, and reconstruction of the skull base.
Infection risk is high, including risk of meningitis, brain abscess and orbital cellulitis. Other complications include traumatic aneurysm, carotid-cavernous fistula, delayed progressive intravascular thrombosis, as well as damage to the globe or optic nerve.
The reconstruction of the skill base is essential to prevent ongoing CSF leak.
This patient was transferred to theatre, for removal of the metal rod under direct vision with endoscopic sinus surgery, with subsequent washout and surgical repair of the base of skull defect.
It is important to perform an angiogram at the time of injury to assess for associated vascular injury. Additionally, a follow up CT angiogram is recommended to assess for the possibility of delayed carotid-cavernous fistula (CT case 8) or post traumatic intracranial aneurysm formation.
References
- Zhang D, Chen J, Han K, Yu M, Hou L. Management of Penetrating Skull Base Injury: A Single Institutional Experience and Review of the Literature. Biomed Res Int. 2017;2017:2838167
- Tabibkhooei A, Aslaninia A, Anousha K. Childhood Transorbital Skull Base Penetrating Injury: Report of 2 Cases and Review of Literature. World Neurosurg. 2019 Nov;131:213-216.
- Sattouf M. Mount Fuji sign. Radiopaedia
- Mattick A, Goodwin P. Mount Fuji sign on CT following trauma. J Trauma. 2005 Jul;59(1):254.
- Heckmann JG, Ganslandt O. Images in clinical medicine. The Mount Fuji sign. N Engl J Med. 2004 Apr 29;350(18):1881
- Nickson C. Eyes Wide Split. LITFL
- Cadogan M. Erich Siedel. LITFL
TOP 100 CT SERIES

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Provisional fellow in emergency radiology, Liverpool hospital, Sydney. Other areas of interest include paediatric and cardiac imaging.

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.