![]()
CT Case 099
A 20-year-old male presents with a tender midline neck mass which has developed over the preceding few days. He was systemically well.
He has never noticed this before and has no significant past medical history.
On examination there is a tender slightly red midline neck mass, approximately 3 x 3cm in size. The mass is fluctuant and moves with swallowing.
CT chest

Describe and interpret the CT scan
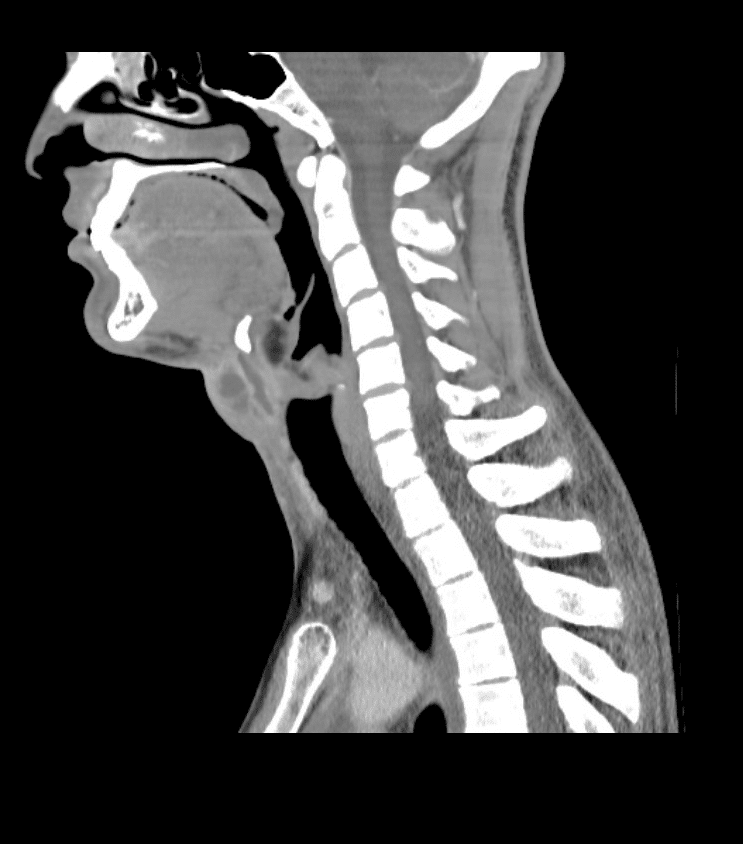
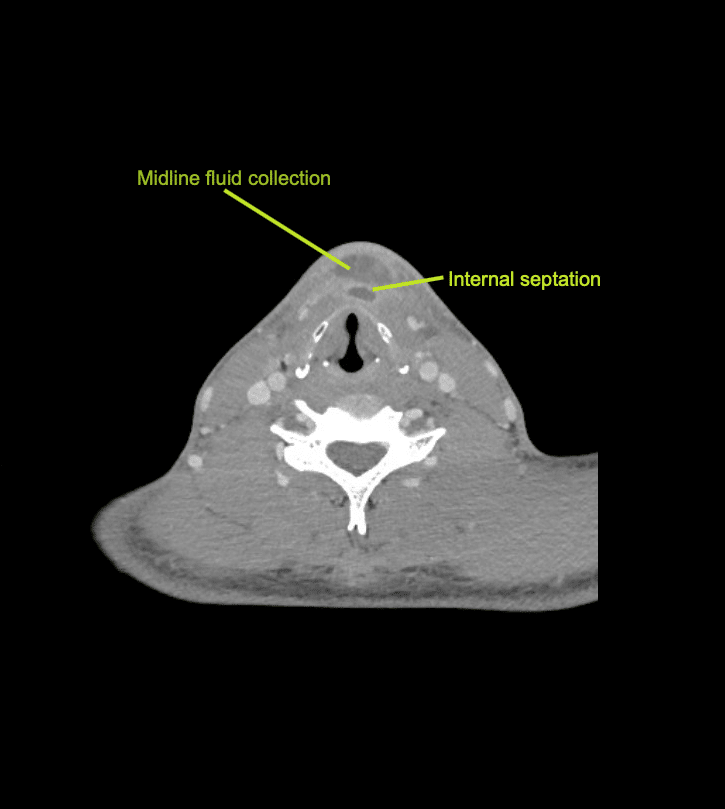
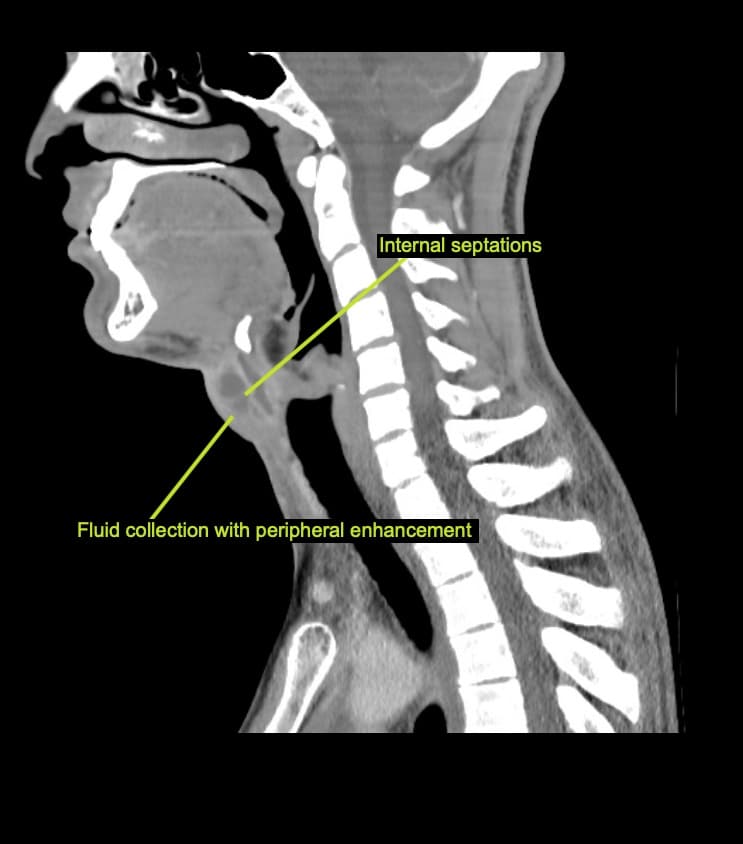
There is a peripherally enhancing midline fluid collection in the infrahyoid region measuring 25 x 15x 15mm.
There are internal septations and mild surrounding fat stranding.
This is in keeping with an infected thyroglossal duct cyst.
Clinical Pearls
When assessing a midline neck mass a differential diagnosis should include;
- Thyroglossal duct cyst
- Dermoid cyst
- Laryngocele
- Ranula
- Ectopic thyroid tissue
- Thyroid mass
On physical exam, a thyroglossal duct cyst can be differentiated from other neck lumps by observing the movement of the cyst when the patient is swallowing or protruding their tongue. If the lump is a thyroglossal duct cyst, it will be seen to move upwards with both of these manoeuvres.
Whereas a thyroid mass will move with swallowing, but not with tongue protrusion.
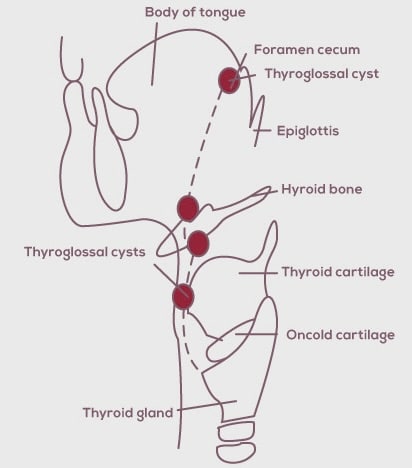
A thyroglossal duct cyst is a congenital abnormality that results from failure of normal obliteration of the thyroglossal duct during development.
The location of a thyroglossal duct cyst can vary. Some are located above the hyoid bone, others between the hyoid bone and thyroid cartilage and others below the sternum or within the tongue.
The majority of thyroglossal duct cysts are located below the level of the hyoid bone, as in this case.
Thyroglossal duct cysts form 70% of all congenital neck anomalies and are the 2nd most common benign lesion after lymphadenopathy. They usually present during childhood (90% before the age of 10 years) as a gradually growing painless fluctuant cervical mass or maybe asymptomatic until they become infected, as in this case.
This case was managed with IV antibiotics (ceftriaxone) and IR guided drainage (3ml of purulent discharge was drained). He was discharged with oral antibiotics and planned for subsequent definitive management with a Sistrunk procedure (removal of the cyst and part of the hyoid bone, as well as a small core of tissue from the hyoid bone all the way to the foramen cecum). Histologic examination is important in all cases, as there is a 1-2% incidence of associated thyroid carcinoma
References
- Walizai T. Thyroglossal duct cyst. Radiopaedia
- Elkins A. Sistrunk Procedure for Thyroglossal Duct Cyst. Thyroid Clinic
- Dermawan JK, Chute DJ. Educational Case: Developmental Neck Masses and Other Neck Tumors. Acad Pathol. 2019 Nov 22;6:2374289519888735.
TOP 100 CT SERIES

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Provisional fellow in emergency radiology, Liverpool hospital, Sydney. Other areas of interest include paediatric and cardiac imaging.