
![]()
CXR Case 027
A 69 year old man presents with slowly worsening dypnoea, raised JVP, peripheral oedema and cyanosis.
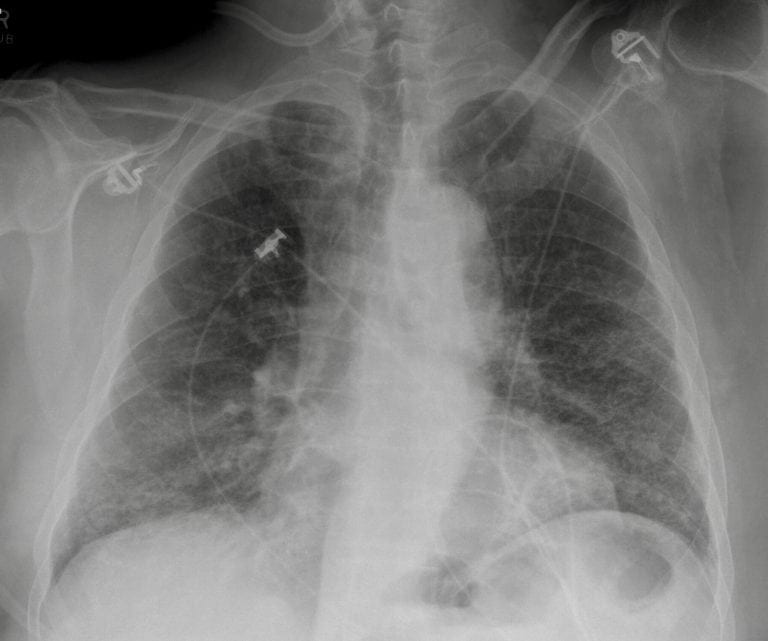
AP CXR 
Fingers

click images to enlarge
Describe and interpret this CXR and clinical image
IMAGE INTERPRETATION
CXR Interpretation:
There is diffuse reticulonodular infiltrate across all lung fields, but most marked in the bases.
*There is loss of volume in both lung fields *
The appearances are consistent with pulmonary fibrosis
Clinical Image:
This is clubbing
CLINICAL CORRELATION
In this case, this patient has developed signs of cor pulmonale secondary to the chronic lung disease.
Bi-basal inspiratory crackles can be commonly miss-labelled as pulmonary oedema, particularly when there is right heart failure.
The presence of clubbing (present in ~50% cases of idiopathic pulmonary fibrosis) should be a strong driver towards considering a primary pulmonary pathology.
CLINICAL PEARLS
Idiopathic Pulmonary Fibrosis has replaced the term ‘cryptogenic fibrosing alveolitis’.
Note: it is only idiopathic when you have excluded the multitude of causes of pulmonary fibrosis, so unless you have taken a full occupational, environmental, smoking and drug exposure history, family history, together with screening for (occult) connective tissue disease, its safer just to call it ‘pulmonary fibrosis‘, and let someone else worry about what sub-type (at least 7 and counting) and what cause!
TOP 150 CXR SERIES
![]()
![]()
![]()
Prof Fraser Brims Curtin Medical School, acute and respiratory medicine specialist, immediate care in sport doc, ex-Royal Navy, academic| Top 100 CXR | Google Scholar | ICIS Course ANZ