
![]()
CXR Case 039
A 74 yo lady is sent in to ED from cardiology clinic with dyspnoea, pleuritic chest pain and fevers. She has a PPM and type II diabetes
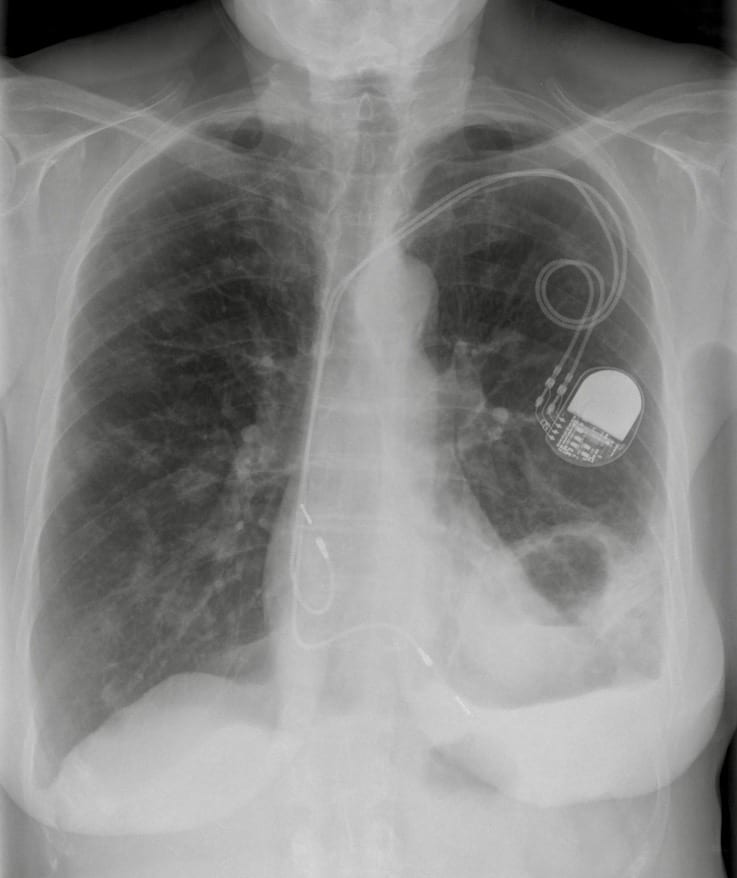
CXR AP 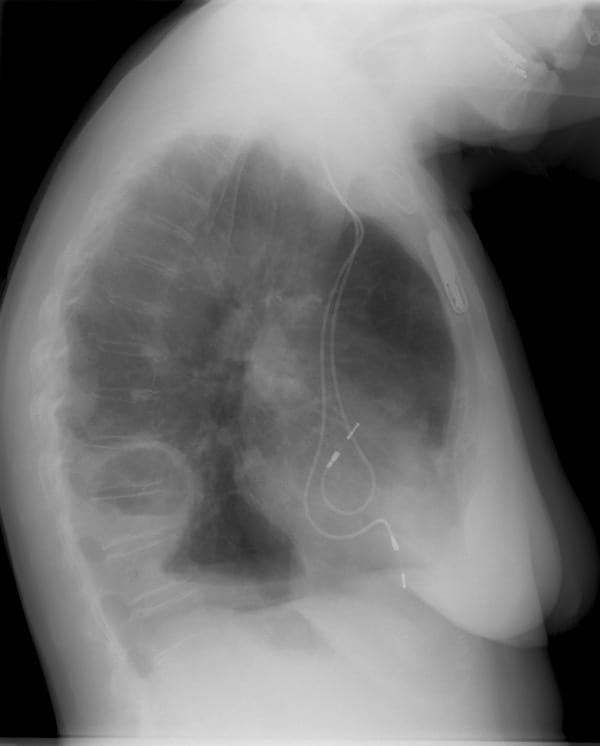
CXR Lateral 
CT Chest
Describe and interpret this Images
IMAGE INTERPRETATION
CXR Interpretation:
There is a left pleural effusion, left basal increased airspace opacification with central lucency and an air fluid level.
*There are multiple different size < 1cm, rounded lesions throughout both lung fields, some with minor cavitation.
Lateral CXR Interpretation:
Lateral X-ray demonstrates a cavity with an air fluid level and associated pleural effusion with loculated fluid superior to the cavity.
CT Chest Interpretation:
CT confirms the presence of a large thick walled fluid containing cavity in the left lower lobe with associated pleural thickening.
*There are small patches of consolidation in the lingula and on the right side.
CLINICAL CORRELATION
This lady has septic emboli causing lung abscess and pleural infection.
*The source of the infection is presumed to be the pacing leads. Staphylococcus aureus was cultured from blood.
CLINICAL PEARLS
One of the major concerns in this case was if the lung abscess was directly communicating with the pleural cavity.
Drainage of the pleura is indicated, drainage of the abscess (with subsequent bronchopleural fistula formation) is not indicated!
TOP 150 CXR SERIES
![]()
![]()
![]()
Prof Fraser Brims Curtin Medical School, acute and respiratory medicine specialist, immediate care in sport doc, ex-Royal Navy, academic| Top 100 CXR | Google Scholar | ICIS Course ANZ