
![]()
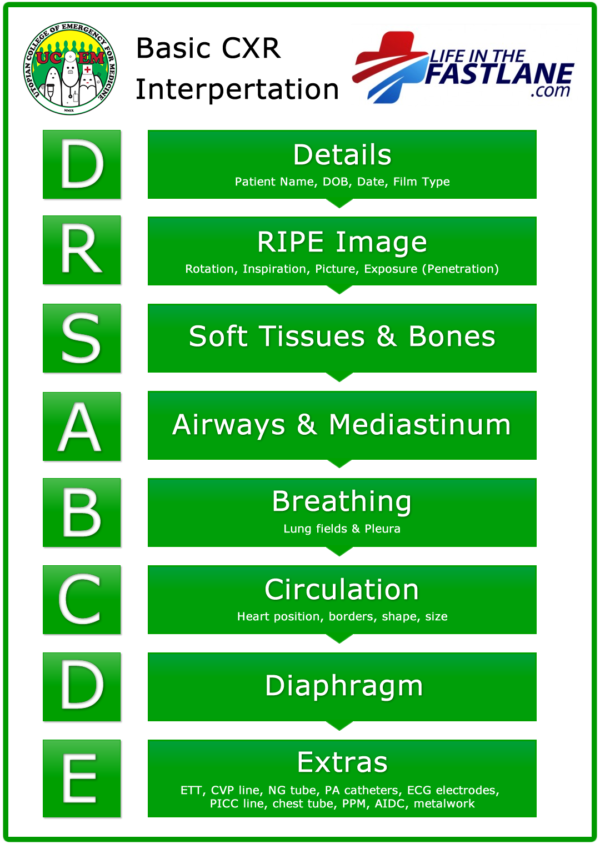
DRSABCDE of CXR Interpretation
Chest X-Rays (CXR) are routine investigation in clinical practice and consequently it is important for medical students and clinician’s alike to know how to interpret them. There are many approaches to CXR interpretation, each trying to ensure that key abnormalities are identified and no area is overlooked. Many people would be familiar with the ABC method to interpreting CXRs.
This is a simple way of approaching CXR, and it works for many people, however some people still struggle using this approach. DRSABCD is a familiar acronym for those who have undertaken First Aid/Basic Life Support courses. Now DRSABCDE can used as a simple, yet comprehensive, approach to CXR interpretation.
D – Details
DETAILS
Before you even begin interpreting a CXR you should have the correct details. This includes;
- Patient name, age / DOB, sex
- Type of film – PA or AP, erect or supine, correct L/R marker, inspiratory/expiratory series
- Date and time of study
R – RIPE (assessing the image quality)
RIPE
Next up, how “ripe” is the image. That is, what is the technical quality of the film?
- Rotation – medial clavicle ends equidistant from spinous process
- Inspiration – 5-6 anterior ribs in MCL or 8-10 posterior ribs above diaphragm, poor inspiration?, hyperexpanded?
- Picture – straight vs oblique, entire lung fields, scapulae outside lung fields, angulation (ie ’tilt’ in vertical plane)
- Exposure (Penetration) – IV disc spaces, spinous processes to ~T4, L) hemidiaphragm visible through cardiac shadow.
S – Soft tissues and bones
SOFT TISSUES/BONES
In CXR interpretation it is common to leave soft tissues until the end.
- Ribs, sternum, spine, clavicles – symmetry, fractures, dislocations, lytic lesions, density
- Soft tissues – looking for symmetry, swelling, loss of tissue planes, subcutaneous air, masses
- Breast shadows
- Calcification – great vessels, carotids
A – Airway & mediastinum
AIRWAY
- Trachea – central or slightly to right lung as crosses aortic arch
- Paratracheal/mediastinal masses or adenopathy
- Carina & RMB/LMB
- Mediastinal width <8cm on PA film
- Aortic knob
- Hilum – T6-7 IV disc level, left hilum is usually higher (2cm) and squarer than the V-shaped right hilum.
- Check vessels, calcification.
B – Breathing
BREATHING
Lung Fields:
- Vascularity – to ~2cm of pleural surface (~3cm in apices), vessels in bases > apices
- Pneumothorax – don’t forget apices
- Lung field outlines – abnormal opacity/lucency, atelectasis, collapse, consolidation, bullae
- Horizontal fissure on Right Lung
- Pulmonary infiltrates – interstitial vs alveolar pattern
- Coin lesions
- Cavitary lesions
Pleura
- Pleural reflections
- Pleural thickening
C – Circulation
CIRCULATION
- Heart position –⅔ to left, ⅓ to right
- Heart size – measure cardiothoracic ratio on PA film (normal <0.5)
- Heart borders – R) border is R) atrium, L) border is L) ventricle & atrium
- Heart shape
- Aortic stripe
D – Diaphragm
DIAPHRAGM
- Hemidiaphragm levels – Right Lung higher than Left Lung (~2.5cm / 1 intercostal space)
- Diaphragm shape/contour
- Cardiophrenic and costophrenic angles – clear and sharp
- Gastric bubble / colonic air
- Subdiaphragmatic air (pneumoperitoneum)
E – Extras
EXTRAS
- ETT, CVP line, NG tube, PA catheters
- ECG electrodes, PICC line, chest tube
- PPM, AIDC, metalwork
Further Reading
- Labelled normal Chest X-ray
- ABC of CXR Interpretation
- Top 150 CXR Quiz
- Chest X-ray for the OSCE
- Dr Eric Strong Vodcast series on CXR Interpretation
Radiology Library
CT, X-ray, Echo, Ultrasound
Prof Fraser Brims Curtin Medical School, acute and respiratory medicine specialist, immediate care in sport doc, ex-Royal Navy, academic| Top 100 CXR | Google Scholar | ICIS Course ANZ