
![]()
ECG Case 077
78 yr old male presents with a 2 day history of lethargy and dizziness. He has a history of ischaemic heart disease, type 2 diabetes, hypertension, and chronic renal failure. His medications include calcium-channel blocker, beta-blocker, and ACE-inhibitor.
He is conscious with systolic BP of 70.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
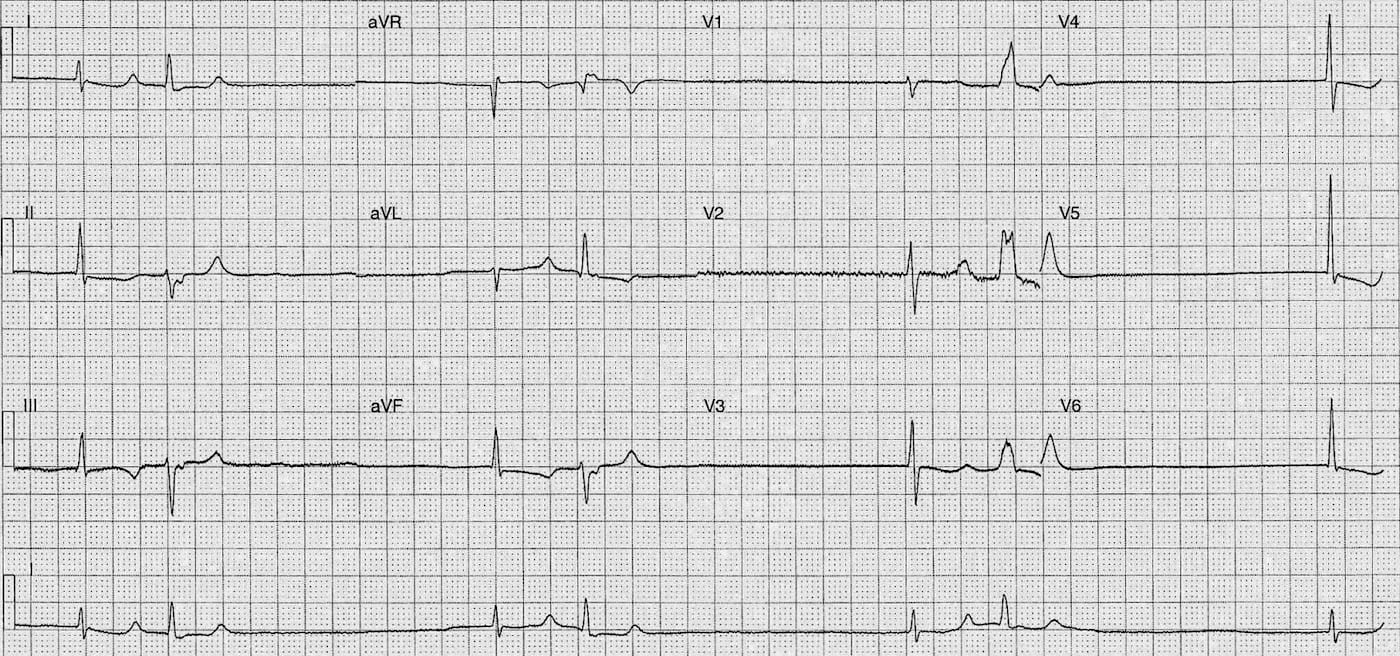
Rate:
- ~42
Rhythm:
- Regularly irregular
- Complexes occurring in paired group
- Flat baseline without atrial activity
Axis:
- 1st Complex in pair
- Normal (70 deg)
- 2nd Complex in pair
- LAD(-45 deg)
Intervals:
- 1st Complex in pair
- QRS – Normal (80ms)
- QT – 520ms
- 2nd Complex in pair
- QRS – Normal in limb leads, Prolonged V1-3 (80-120ms)
- QT – 440ms
Segments:
- 1st Complex in pair
- ST Depression leads II, aVF
- 2nd Complex in pair
- Minimal ST elevation lead aVR
Additional:
- 1st Complex in pair
- T wave inversion II, III, aVF
- Biphasic T lead V3
- 2nd Complex in pair
- RsR’ Morphology V1-3
- Inverted notching terminal portion QRS II, III, aVF also positive notching aVL
- ? Retrograde P waves ? Secondary to conduction delay
Interpretation:
- Escape bigeminy
- In setting of sinus arrest / sinus exit block
- Non-specific ST / T wave changes
Differential of causes:
- Ischaemia
- Electrolyte disturbance
- Acid-base disturbance
- Cardiotoxic drugs
- Sinus node dysfunction
- Hypothermia
- Multifactorial combination of above
WHAT HAPPENED NEXT?
Bloods showed:
- Acute on chronic renal failure
- Metabolic acidosis – pH 7.0 Bicarb 7.0
- K 6.0
Treated with isoprenaline, sodium bicarb, cessation of cardiotoxic medication, and dialysis.
Following acute episode found to have sinus pauses on telemetry necessitating pacemaker insertion.
FURTHER READING
LITFL
- ECG Library – Sinus Arrest
- ECG Library – Sinoatrial exit block
TOP 100 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |