
![]()
ECG Case 083
63 yr old female who presented with a 3 day history of colicky right upper quadrant abdominal pain. She is normally fit and well and has no prior past medical history.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
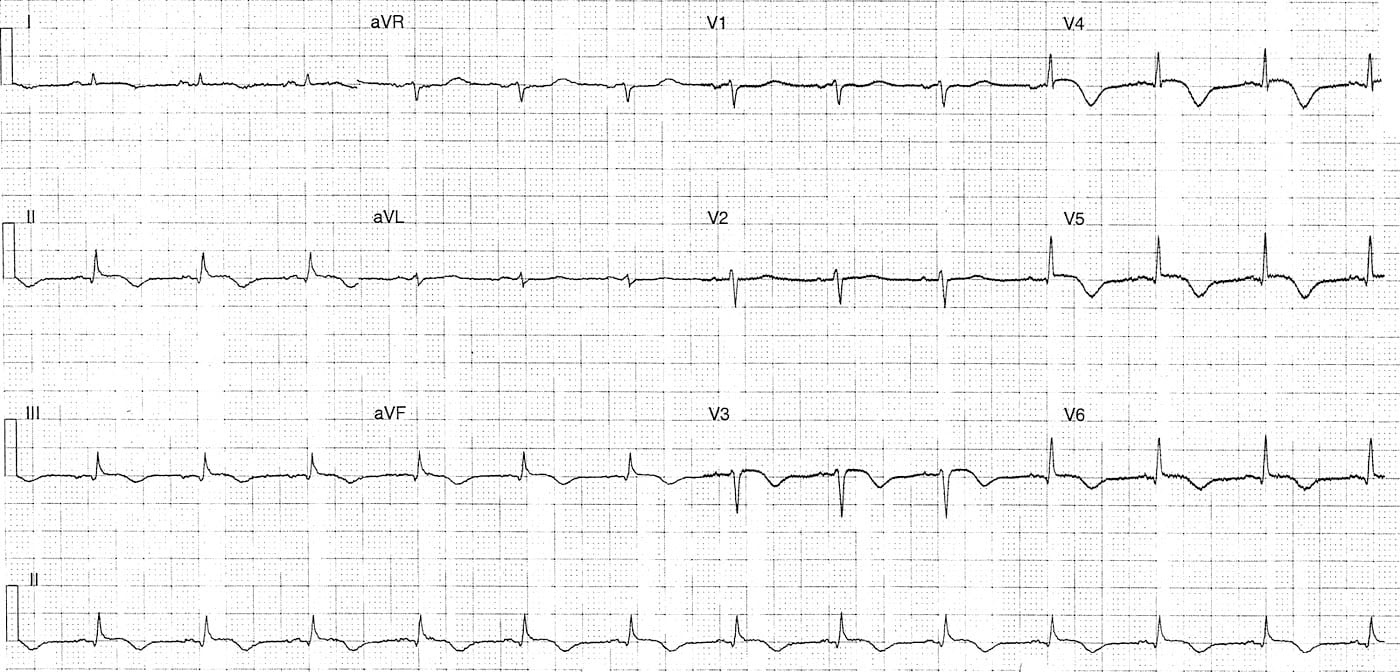
Rate:
- 78 bpm
Rhythm:
- Regular
- Sinus rhythm
Axis:
- Normal
Intervals:
- PR – Normal (~160ms)
- QRS – Normal (80ms)
Additional:
- ST Elevation leads V2-5 (~1mm)
- Subtle ST elevation leads II, III, aVF, V6
- T wave inversion leads II, III, aVF, V3-6
- Absence of ST depression
- Low voltage P wave with notching in lead II
Interpretation:
- Diffuse ST and T wave changes
DDx includes:
- ACS
- Demand ischaemia secondary to sepsis
- Cardiomyopathy – acute vs chronic
- Electrolyte abnormality / Acid-base disturbance
OUTCOME
This patient had no history of chest pain, nil pre-existing medical condition and was not significantly unwell from her assumed cholecystitis. Vital signs and electrolytes were normal.
She was admitted under the cardiology team for further investigation of ECG abnormalities with surgical consultation for management of cholecystitis.
The patient had raised cardiac biomarkers and underwent angiography.
Angiogram showed no coronary vessel disease but Takotsubo pattern cardiomyopathy, EF 35-40%. The patient was commenced on beta-blocker, ACE and diuretic therapy and underwent elective cholecystectomy once cardiac function and follow-up echo returned to normal.
REFERENCES
Check out some great cases from Dr Smith’s ECG blog on Takotsubo here:
LITFL
- ECG Library – Takotsubo Cardiomyopathy
- Top 100 Ultrasound – Case 091
TOP 100 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |

This ECG seems leads reversal, positive T waves in aVR and V1?