
![]()
Takotsubo Cardiomyopathy
Overview
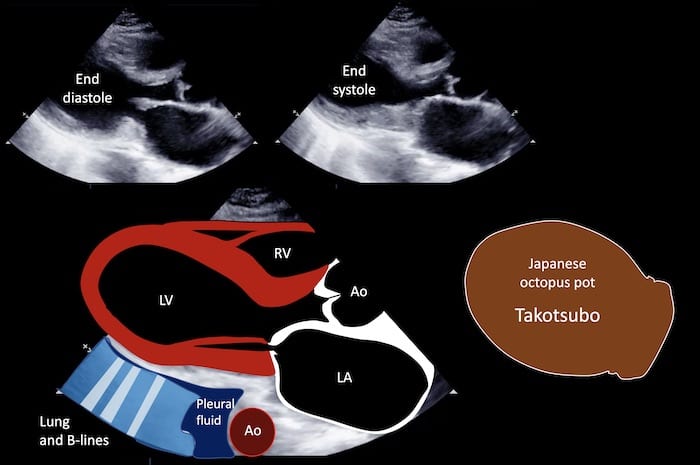
- Transient wall motion abnormality of the left ventricular apex associated with severe emotional or physical stress that usually resolves completely
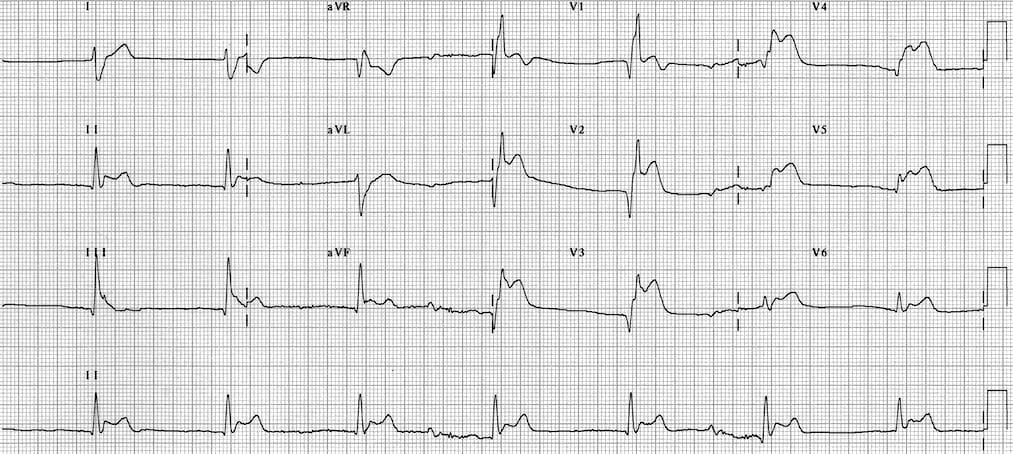
- Produces ischaemic chest pain, ECG changes +/- elevated cardiac enzymes in patients with normal coronary arteries on angiography
- The presentation often mimics a STEMI and angiography is required to definitively differentiate the two conditions
Mayo Clinic diagnostic criteria
- Transient dyskinesis of the LV apical and/or midsegments
- Regional wall motional abnormalities beyond a single epicardial vascular distribution
- Absence of coronary artery stenosis > 50% of culprit lesion
- New ECG changes (ST elevation or T wave inversion) or moderate troponin rise
- Absence of phaeochromocytoma and myocarditis
Also known as stress cardiomyopathy, apical ballooning syndrome, or broken heart syndrome.
History of Takotsubo
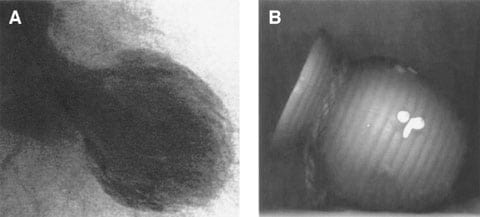
Originally described in Japan in 1990, the condition is named after the takotsubo pot, a traditional basket used in Japan to catch octopi. In TCM, apical dyskinesia and subsequent ballooning creates an LV appearance remarkably similiar to this octopus pot.

Pathophysiology
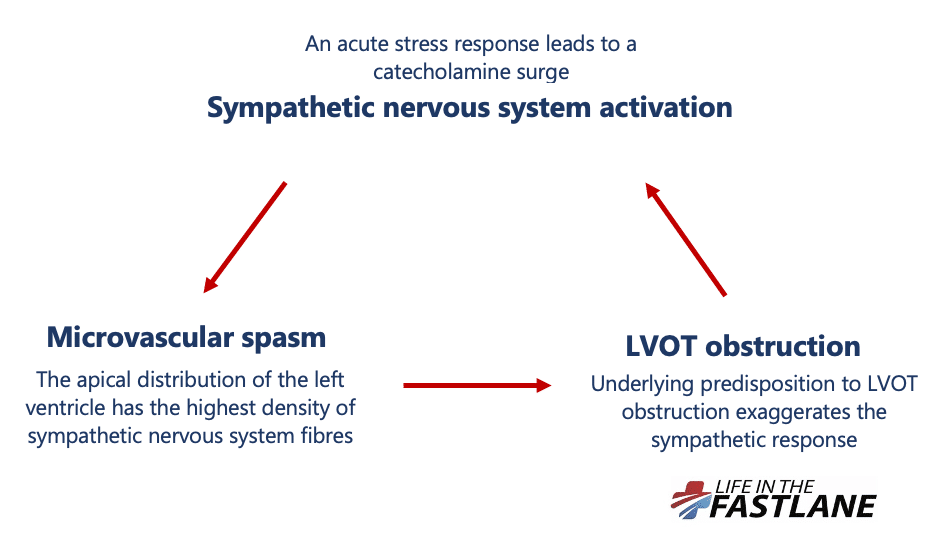
Pathophysiology is thought to be related to a combination of sympathetic nervous system activation, microvascular spasm, and underlying LVOT obstruction:
- An acute stress response leads to a catecholamine surge
- Ensuing sympathetic nervous system activation causes microvascular spasm. The apical distribution of the left ventricle has the highest density of sympathetic nervous system fibres which may explain the characteristic regional wall dyskinesia.
- In at least one-third of cases, there is a degree of underlying left ventricular outflow tract (LVOT) obstruction, which increases LV workload, worsening sympathetic nervous system activation and apical dyskinesis. These patients usually have more severe disease and a poorer prognosis
The condition can be prevented in a laboratory by cardiac sympathectomy, and similar cardiac histopathological features are seen in patients who have suffered a subarachnoid haemorrhage.
Clinical significance
- 90% of cases worldwide occur in post-menopausal women, usually associated with sudden emotional stress. Cases in men are more likely to be associated with physical stress
- Takotsubo cardiomyopathy is difficult to distinguish from STEMI in the ED, and no ECG criteria can be safely used to differentiate between the two conditions. If in doubt, you should activate your local code STEMI protocol
- Takotsubo has a better prognosis than STEMIs with a similar ECG but it is certainly not benign
- Treatment is largely supportive, and LV function usually spontaneously returns within 21 days of onset
- Anticoagulation should be initiated in patients with large areas of cardiac hypokinesis, as they are at high risk of cerebrovascular thromboembolic events
Related Topics
References
- ClinicalCases Blogspot with Dr Ves: Takotsubo cardiomyopathy broken heart syndrome
- Akashi YJ, Goldstein DS, Barbaro G, Ueyama T. Takotsubo cardiomyopathy: a new form of acute, reversible heart failure. Circulation. 2008;118(25):2754-2762
- Abdulla I, Ward MR. Tako-tsubo cardiomyopathy: how stress can mimic acute coronary occlusion. Med J Aust. 2007;187(6):357-360.
- Banning et al. Takotsubo cardiomyopathy BMJ 2010;340:c1272.
- Virani SS, Khan AN, Mendoza CE, Ferreira AC, de Marchena E. Takotsubo cardiomyopathy, or broken-heart syndrome. Tex Heart Inst J. 2007;34(1):76-79.
- Komamura et al. Takotsubo cardiomyopathy: Pathophysiology, diagnosis and treatment. World J Cardiol. 2014 Jul 26; 6(7):602-609
- Geisen WR, Rosse C, Menon S, Rudick S. Trump Cardiomyopathy: A New Form of Takotsubo Cardiomyopathy J Card Fail. 2020
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.