
![]()
ECG Case 084
89 yr old female presents with chest pain. She has a history of 2nd degree AV block with PPM in-situ.
Serially ECGs were recorded
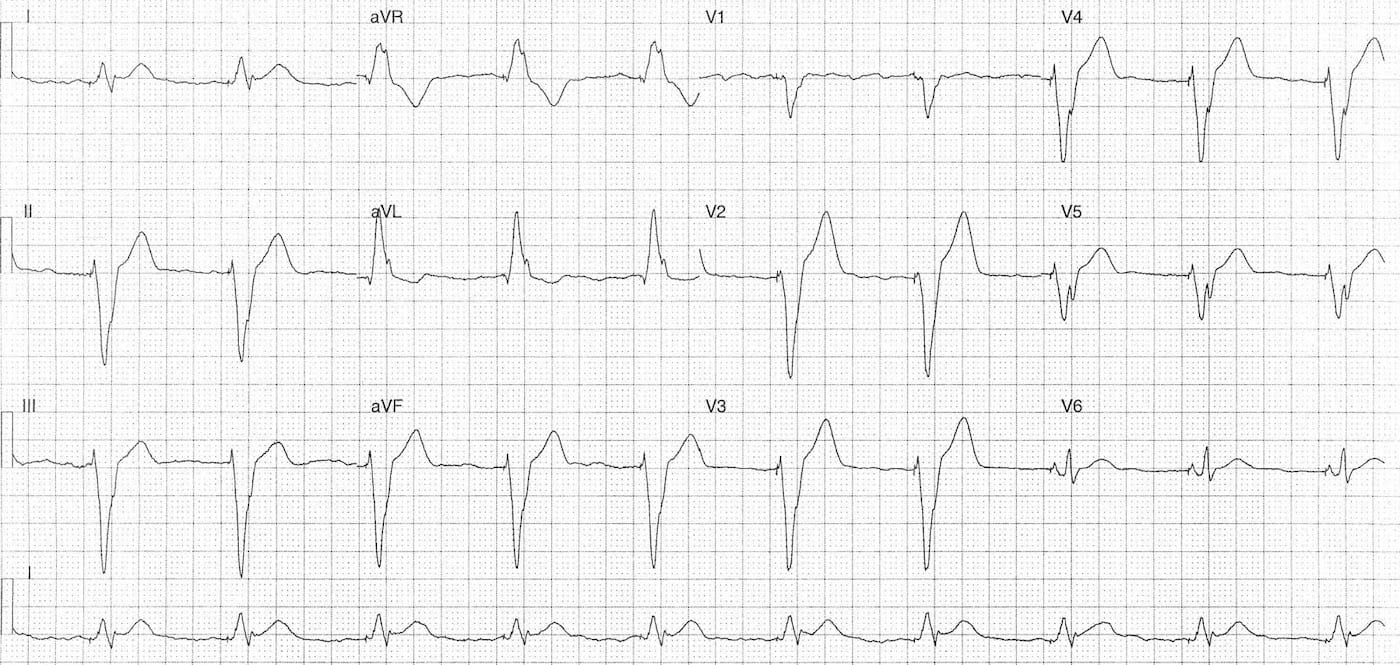
ECG 1; on arrival pain 3/10
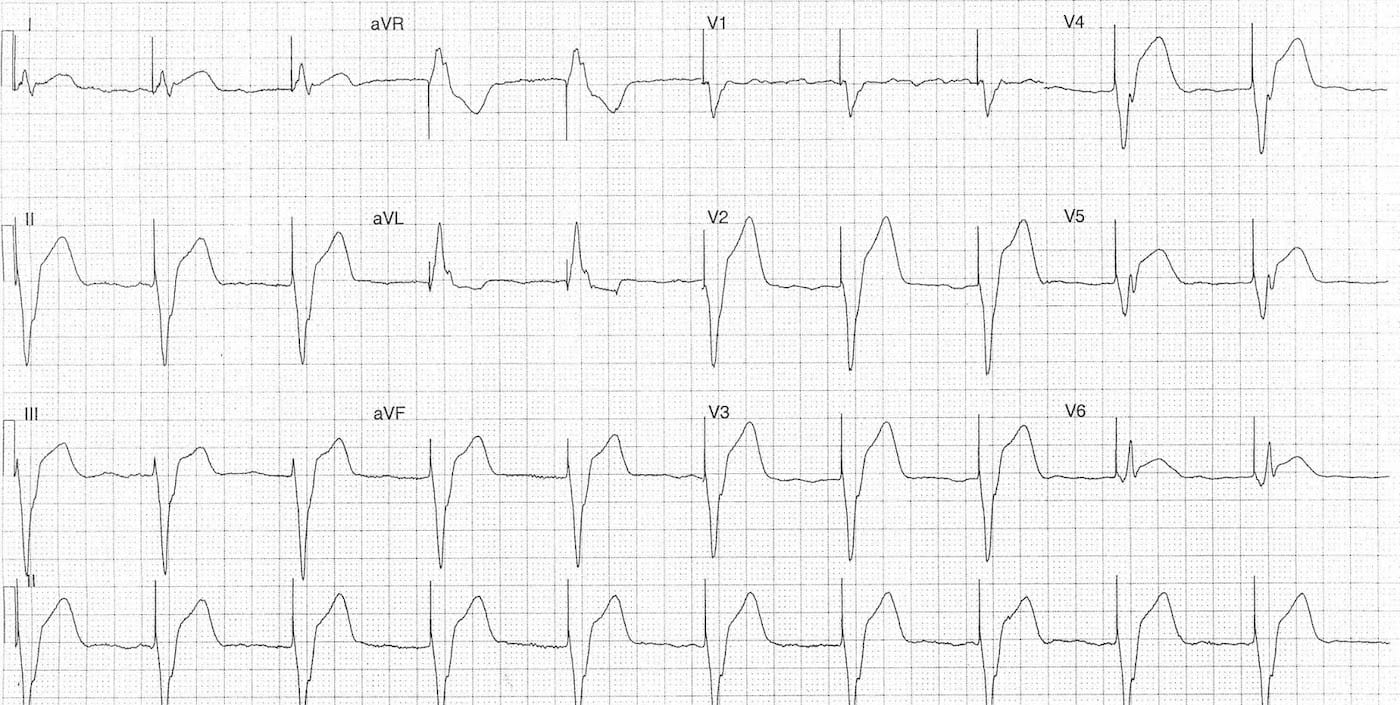
ECG 2; 60 mins later with a further bout of chest pain 8/10
Describe and interpret these ECGs
ECG ANSWER – ECG 1
Key features:
- Rate 60 bpm
- Regular V-paced rhythm
- LBBB Morphology
- Discordant ST / T wave changes
- T waves in leads V2-4 appear prominent
- Concordant ST elevation in lead I with a positive QRS
- Subtle and easy to miss
ECG ANSWER – ECG 2
Key features:
- Rate 60 bpm
- Regular V-paced rhythm
- LBBB Morphology
- Significant progression of ST and T wave changes
- Massive ST elevation (>5mm) in leads V2-4 also proportionately >25% of QRS depth
- Discordant ST elevation in leads II, III, aVF, V5
- Significantly more pronounced than on previous ECG
- Concordant ST elevation in leads I and V6
INTERPRETATION and OUTCOME
Sgarbossa positive ECG’s
- Dynamic and progressive ST segment changes
- Underlying V-paced rhythm with LBBB morphology
The patient was discussed with the cardiology team and taken for angiography.
This showed an acute mid LAD occlusion treated with a bare metal stent. Post angiography echo showed moderate systolic and diastolic dysfunction. She was discharged following a 2 day in-patient stay.
FURTHER READING
- STEMI in the context of LBBB – by Stephen Smith at EP Monthly
- ECG Library – Sgarbossa Criteria
- Sgarbossa rule update from Sgarbossa et al – American Heart Journal 2013
- ECG Quest – Positive Sgarbossa criteria
- Excellent ECG cases exploring ischaemia in the context of LBBB – Dr Smith’s ECG Blog
- ECG Library – Left Bundle Branch Block
- Sgarbossa EB. Sgarbossa’s Criteria for MI in Left Bundle Branch Block. MDCalc
TOP 100 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |