
![]()
ECG Case 086
70 yr old male who presented with general lethargy and postural dizziness. He has a collapse the evening prior and recently had a diarrhoeal illness.
His medications include warfarin, metoprolol, frusemide, allopurinol, colchicine and digoxin.
Vital signs on arrival in the Emergency Department were:
- GCS 14
- BP 78/36
- RR 16
- Temp 36.2 C
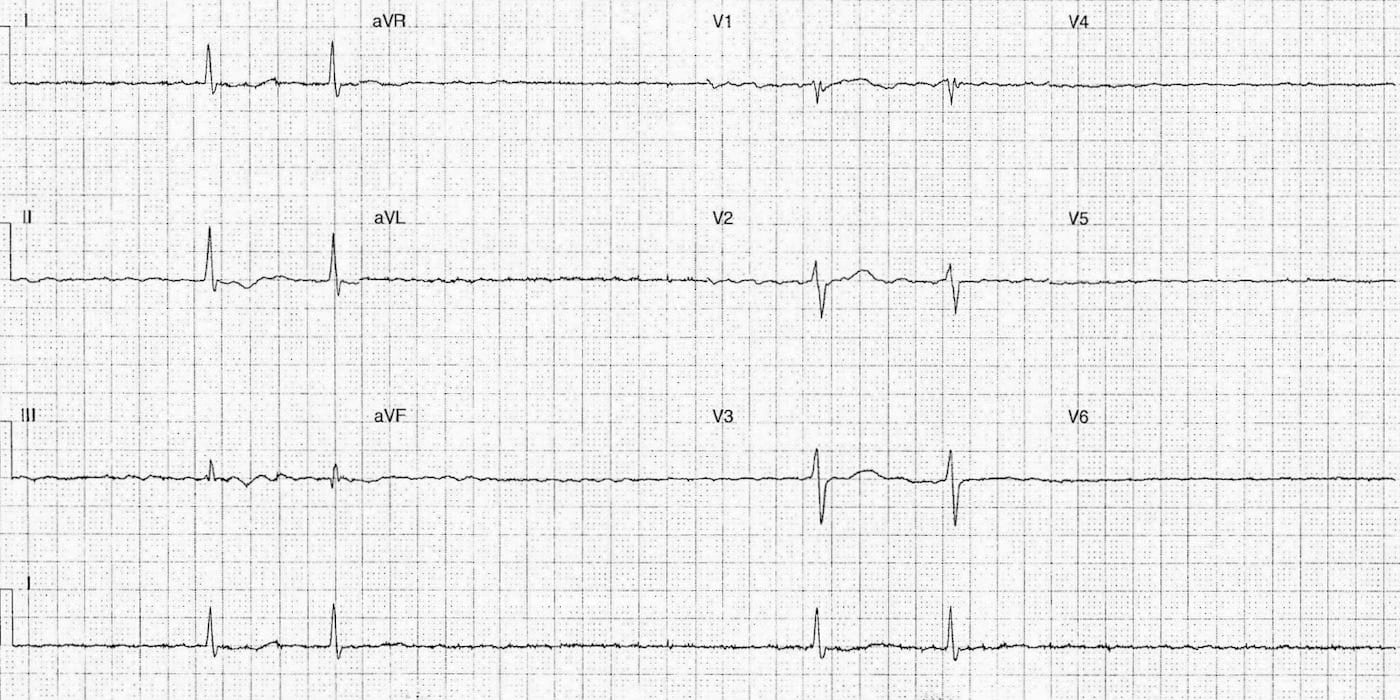
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Rate:
- Mean ventricular rate 24 bpm
Rhythm:
- Pair ventricular beats without fixed R-R intervals
- Absent P waves
- Regularly undulating baseline best seen lead aVL
Axis:
- Normal
Intervals:
- QRS – Prolonged (120ms)
- QT – 580ms (measured in V2 but T wave end difficult to see in other leads)
Additional / Segments:
- Paucity of QRS complexes
- Nil ventricular beats seen in leads aVR, aVL, aVF, V4-6
- T wave inversion leads II and III
Interpretation:
- Severe bradycardia
- Atrial fibrillation
- Associated hypotension and altered GCS
General differentials for this ECG would include:
- Sinus node dysfunction
- Ischaemia
- Hypothermia
- Drug toxicity – calcium channel blockers, beta blockers, digoxin
- Electrolyte abnormality
Our patient has a normal core temperature, is on two potential culprit drugs metoprolol and digoxin and has an underlying dysrhythmia (chronic AF).
OUTCOME
Thankfully the patient responded quickly to a bolus of atropine and iv crystalloid whilst an urgent VBG was obtained and external pacing pads were applied.
The patient had a normal potassium, calcium, magnesium and essentially normal pH.
Treated with 2 vials of digoxin Fab with consistent improvement in heart rate and blood pressure following Fab therapy.
Further bloods revealed new renal impairment likely secondary to recent GI illness and nephrotoxic drugs. The patient was admitted to the HDU for ongoing cardiac monitoring and iv fluid replacement. His renal function improved within 24 hours, digoxin was ceased and his medications were revised to remove unnecessary and potentially toxic drugs.
FURTHER READING
- ECG Library – Digoxin Toxicity
- CCC – Digoxin Toxicity
- CCC – Calcium, Digoxin Toxicity and ‘Stone Heart’ Theory
TOP 100 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |