
![]()
ECG Case 085
56 yr old male who present with 2 hours of chest pain. Past history of hypertension and smoking. The ECG’s were performed 15 mins apart with ongoing chest pain.
ECG 1; On arrival to ED
ECG 2; 15 mins following ECG 1
Describe and interpret this ECG
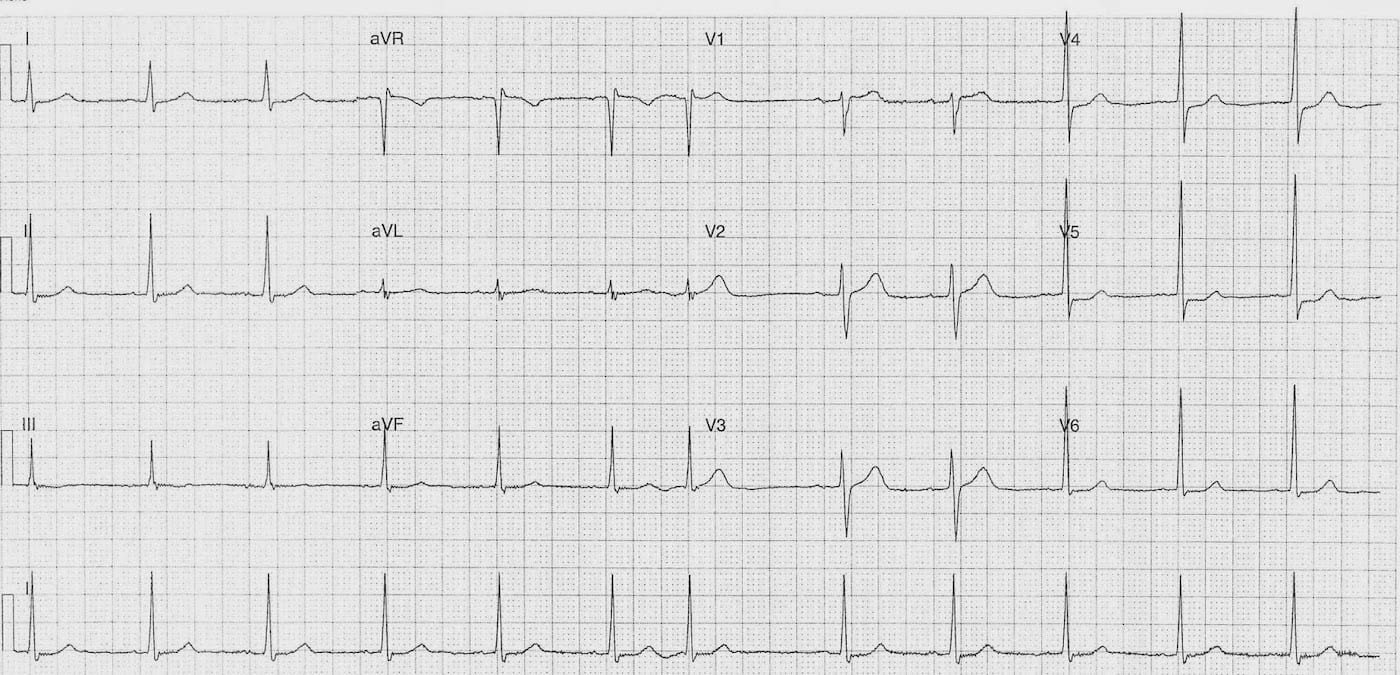
ECG ANSWER – ECG 1
Rate:
- 72 bpm
Rhythm:
- Sinus rhythm
- Single PAC (Complex #7)
Axis:
- Normal
Intervals:
- PR – Normal (160ms)
- QRS – Normal (100ms)
- QT – 360ms
Segments:
- ST Depression leads I, V4-6
Interpretation:
- Lateral ST segment depression
- Given associated Hx of chest pain ischaemia is the main concern
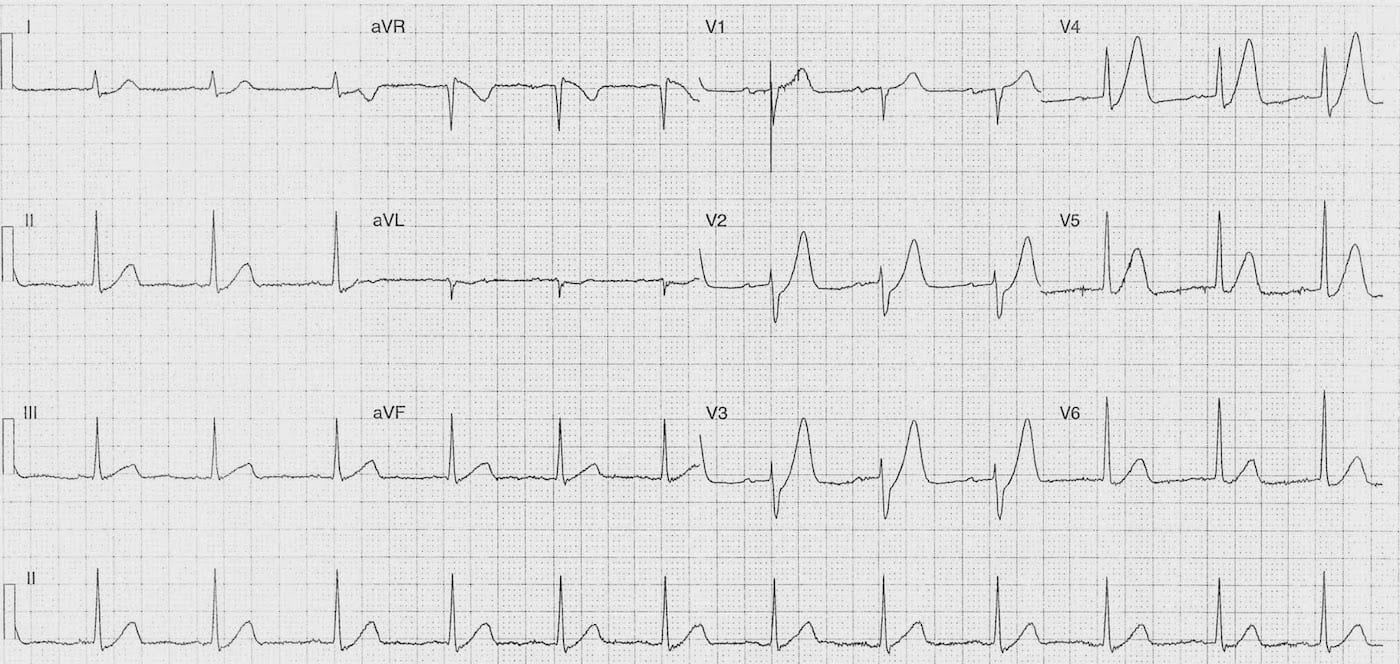
ECG ANSWER – ECG 2
Rate:
- 72 bpm
Rhythm:
- Regular
- Sinus rhythm
Axis:
- Normal
Intervals:
- PR – Normal (180-200ms)
- QRS – Normal (80ms)
- QT – 360ms
Segments:
- ST Depression leads I, II, aVL, V2-6
- ST Elevation lead aVR (~1mm)
Additional:
- Markedly prominent T waves leads I, V2-6
Interpretation:
- De Winter T Wave Pattern
- Suggests acute LAD lesion requiring emergent reperfusion
- Dynamic ECG changes compared with previous ECG
OUTCOME
The ECG changes were recognised by the treating team. The patient was taken for emergency PCI which showed:
- LAD – 100% Occlusion – 2 x stents inserted
- RAC – 30% proximal stenosis
Post stent echocardiogram showed:
- Mild systolic dysfunction
- Akinesis of anterior septum and apical region
- LVEF ~40-45%
The patient was discharged after a 4 day in-patient stay.
I think there are two key learning points from this case:
- The need for serial ECG’s
- Recognition of De Winter’s T Wave Pattern
FURTHER READING
- ECG Library – De Winter T waves
- Eponymictionary – Robbert Jan de Winter
TOP 100 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |