
![]()
ECG Case 103
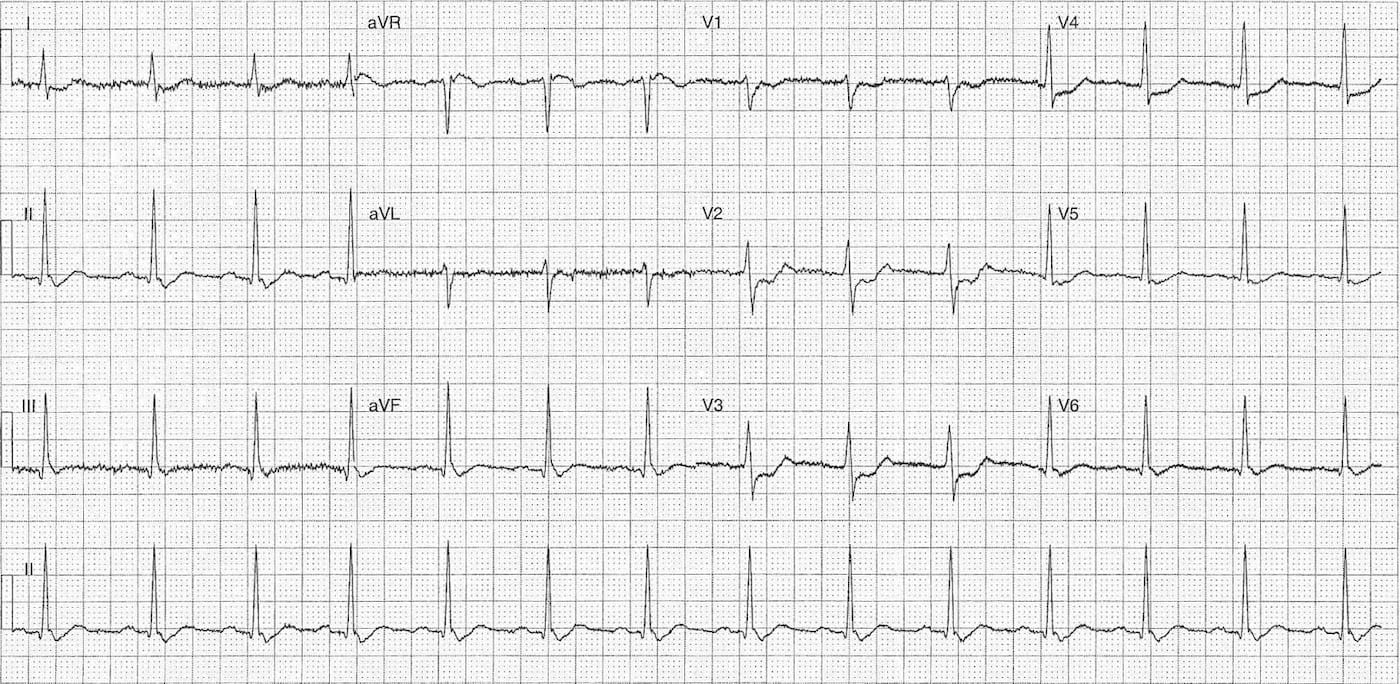
53 year old male presenting with central chest pain for 2 hours, ongoing at time of recording
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Rate:
- ~84 bpm
Rhythm:
- Regular
Axis:
- Normal (~75 deg)
Intervals:
- PR – Normal (200ms)
- QRS – Normal (100ms)
- QT – 360ms (QTc Bazett ~ 425 ms)
Segments:
- ST Elevation lead aVR ~0.5mm
- ST Depression
- Horizontal leads V2-V4
- Concave leads II, aVF, V5-V6
Additional:
- T wave inversion lead V1
- Flat T waves II, III, aVF, aVL, V5, V6
- Notching terminal portion QRS complex leads II, V5, V6
- R/S Ratio V2=0.85
Interpretation:
Highly suspicious ECG for Posterior STEMI
- Flat right precordial ST depression
- Prominent R wave V2, although R/S <1
- Inferolateral ST depression
- Patient c/o acute chest pain
CLINICAL OUTCOME
The patient had posterior leads (V7-9) performed, ECG below.
You can see leads V1 & V3 have been moved to the posterior region and re-labelled as V7 & V9. This configuration is due to our local lead set up which uses only two physical leads with multiple connectors on each to record the twelve lead.

As you can see there is ST elevation in lead V7 (1mm) and V9 (~0.5mm) which is diagnostic of an isolated posterior infarction.
The patient was transferred for urgent coronary angiography & PCI.
His angiography showed:
- Left main – irregularities
- Left anterior descending – 40-50% mid vessel stenosis
- Left circumflex – proximal occlusion
- Right coronary – proximal occlusion with bridging collaterals
- Ventriculogram – normal
His proximal circumflex lesion was stented acutely, and he was discharged following a 4 day in-patient stay.
CLINICAL PEARLS
Mirror Test
Well with a paper ECG you turn it upside down and look through the back of the ECG. Through the magic of computer technology we can do the same with our ECG here, image below.

We can now see ST elevation in these leads with a deep Q and negative T wave similar to the actual posterior lead morphology.
I would recommend people have a read of the great post on EMS 12-Lead blog about these morphology changes as they raise several excellent points about the traditional morphological diagnostic criteria for posterior STEMI.
More on Posterior STEMI
- ECG Library – Posterior Myocardial Infarction
- EMS 12-Lead – Clinical case [Must read review with some ‘mythbusting’ around the ‘traditional’ ECG morphology in posterior STEMI]
- Dr Smith’s ECG Blog – Posterior STEMI related posts –
- Dr Ken Grauer’s ECG Interpretation Blog – Case 1 and Case 2 with posterior involvement
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |