
![]()
ECG Lead positioning
The ECG is one of the most useful investigations in medicine. Electrodes attached to the chest and/or limbs record small voltage changes as potential difference, which is transposed into a visual tracing
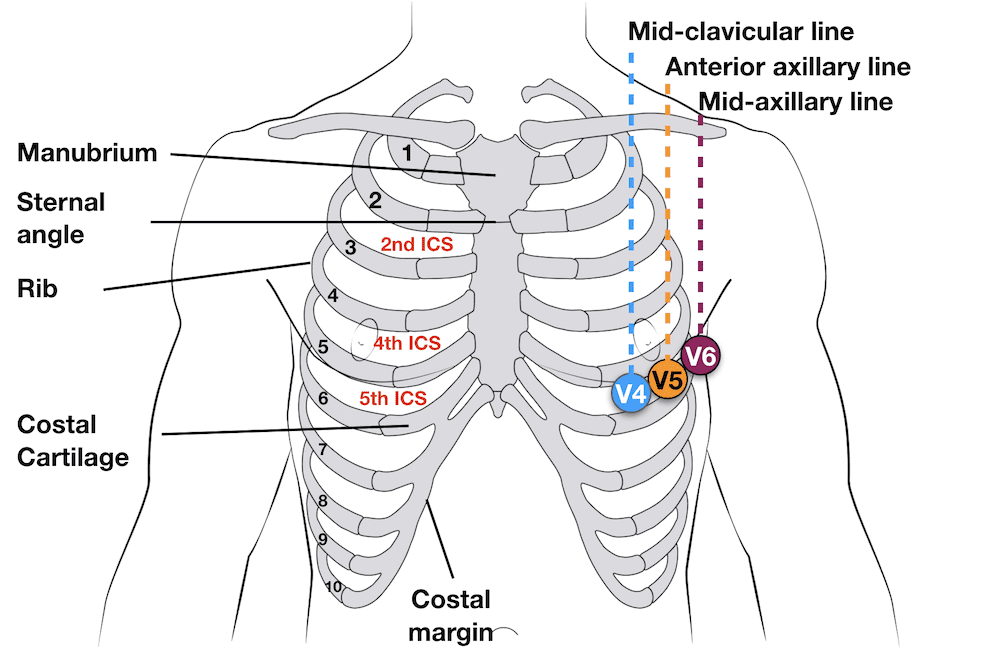
Basic landmarks
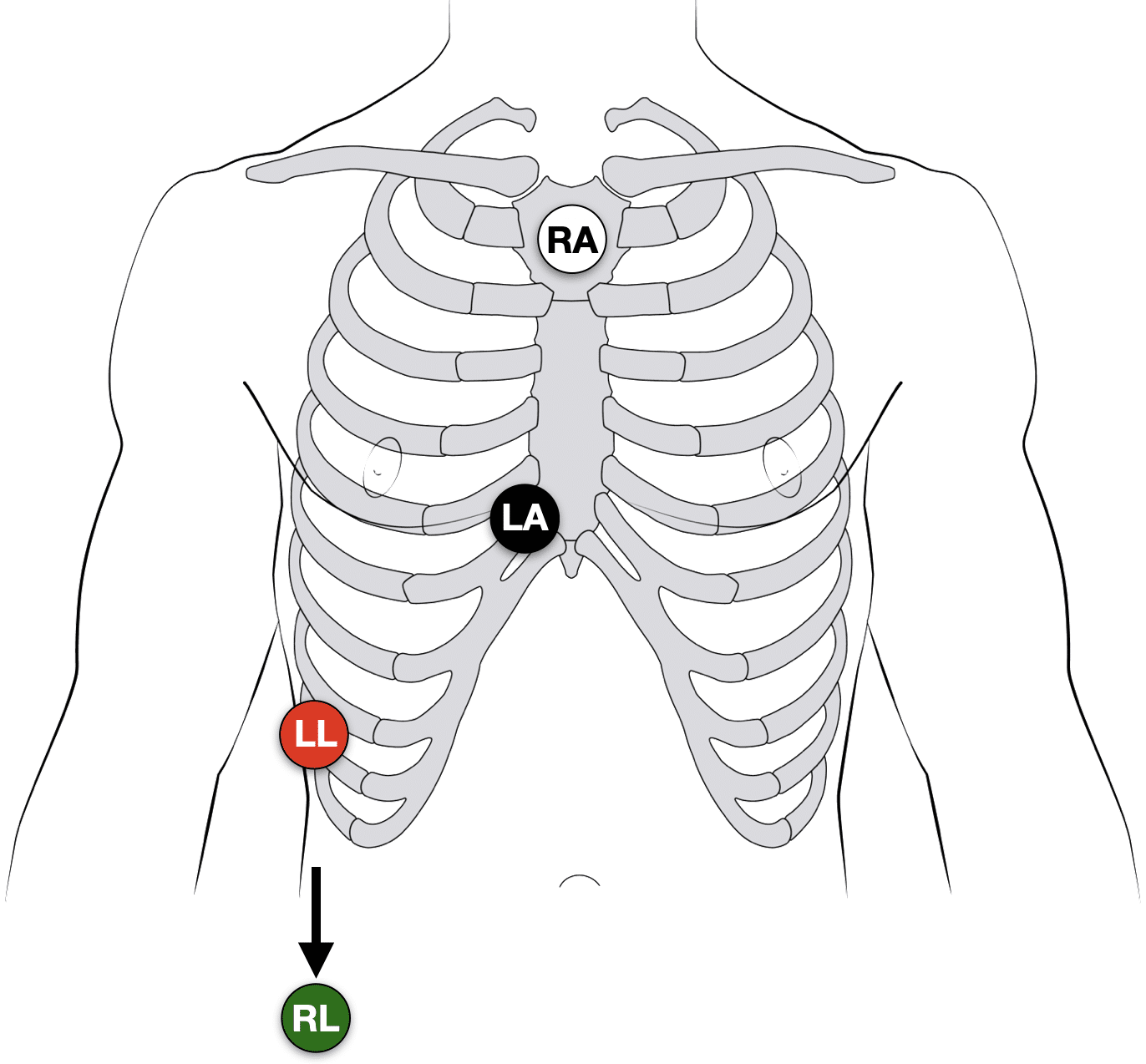
3-electrode system
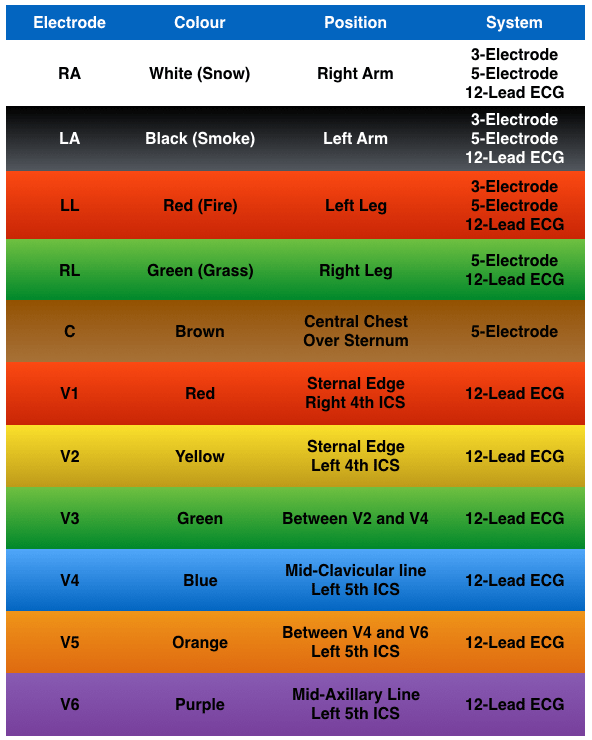
- Uses 3 electrodes (RA, LA and LL)
- Monitor displays the bipolar leads (I, II and III)
- To get best results – Place electrodes on the chest wall equidistant from the heart (rather than the specific limbs)

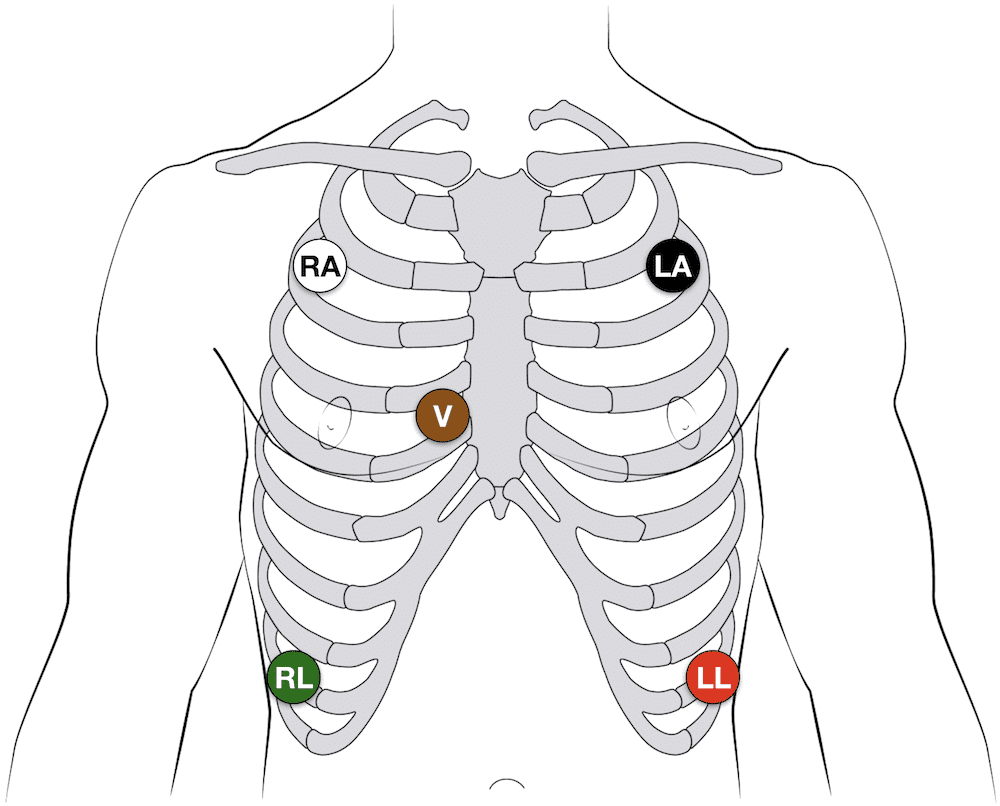
5-electrode system
- Uses 5 electrodes (RA, RL, LA, LL and Chest)
- Monitor displays the bipolar leads (I, II and III)
- AND a single unipolar lead (depending on position of the brown chest lead (positions V1–6))
12-lead ECG
- 10 electrodes required to produce 12-lead ECG
- 4 Electrodes on all 4 limbs (RA, LL, LA, RL)6 Electrodes on precordium (V1–6)
- Monitors 12 leads (V1–6), (I, II, III) and (aVR, aVF, aVL)
- Allows interpretation of specific areas of the heart
- Inferior (II, III, aVF)Lateral (I, aVL, V5, V6)Anterior (V1–4)
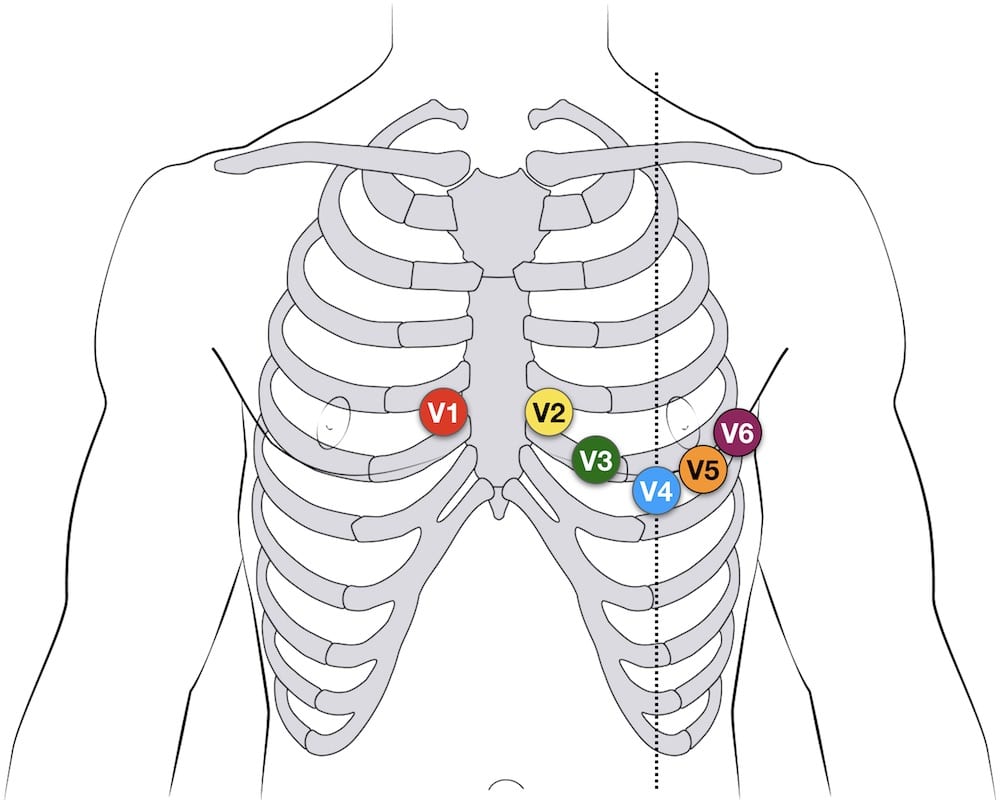
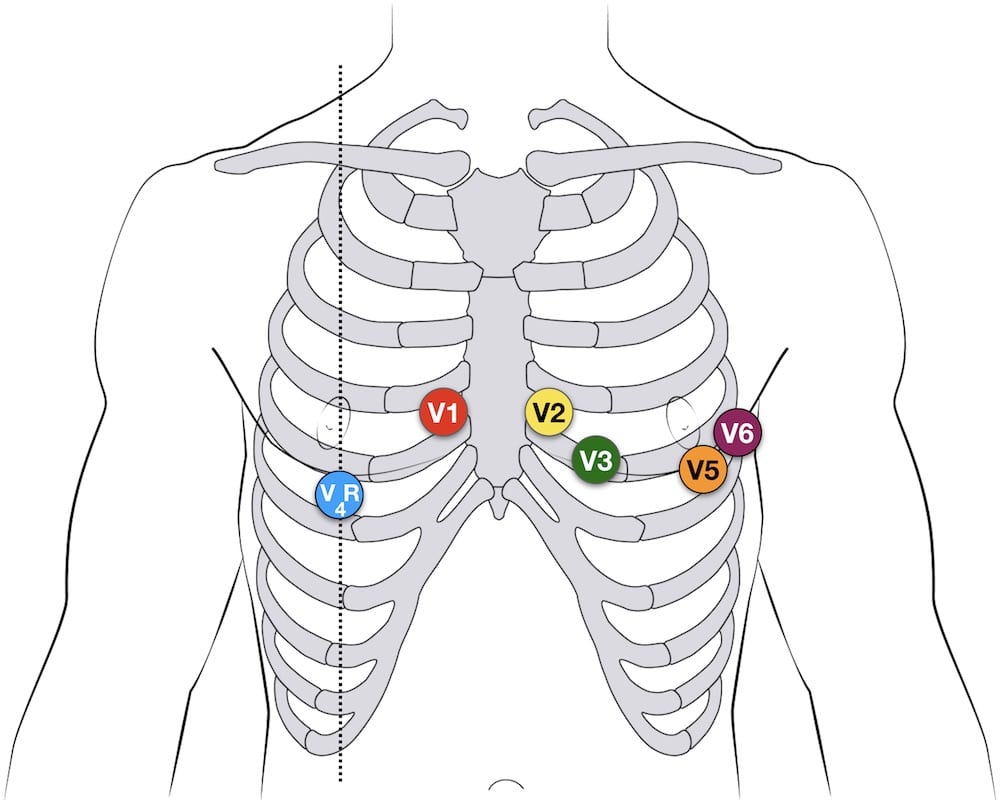
12-lead Precordial lead placement
- V1: 4th intercostal space (ICS), RIGHT margin of the sternum
- V2: 4th ICS along the LEFT margin of the sternum
- V4: 5th ICS, mid-clavicular line
- V3: midway between V2 and V4
- V5: 5th ICS, anterior axillary line (same level as V4)
- V6: 5th ICS, mid-axillary line (same level as V4)
Additional Lead placements
Right sided ECG electrode placement
There are several approaches to recording a right-sided ECG:
- A complete set of right-sided leads is obtained by placing leads V1-6 in a mirror-image position on the right side of the chest (see diagram, below).
- It can be simpler to leave V1 and V2 in their usual positions and just transfer leads V3-6 to the right side of the chest (i.e. V3R to V6R).
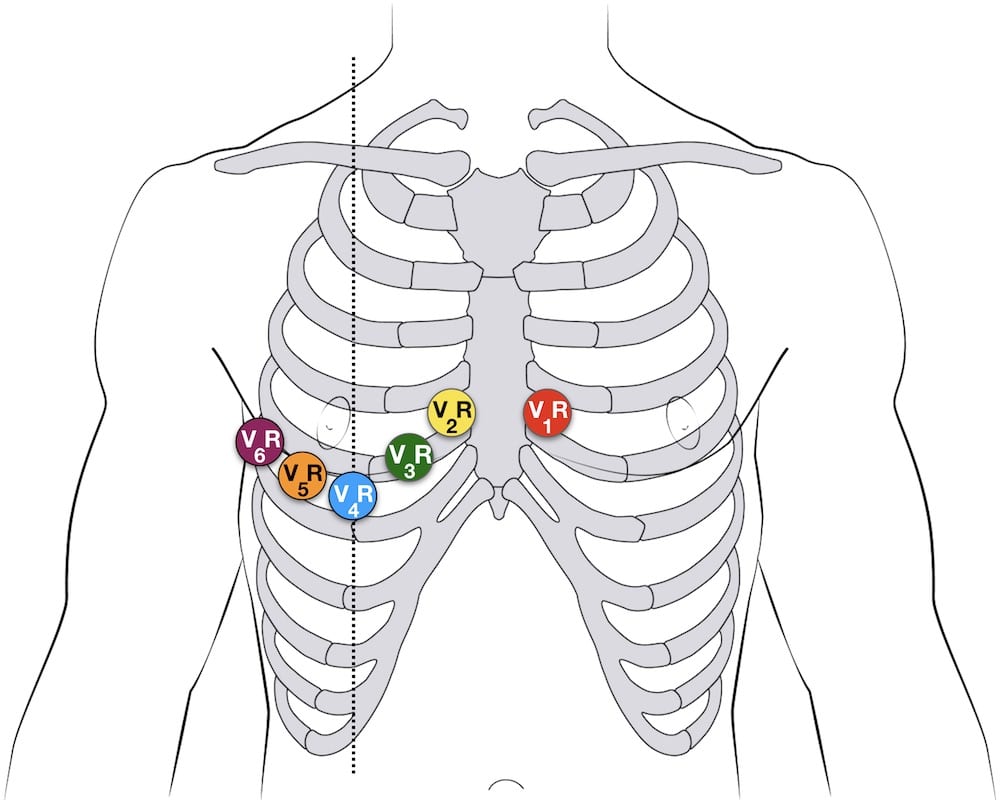
- The most useful lead is V4R, which is obtained by placing the V4 electrode in the 5th right intercostal space in the mid-clavicular line.
- ST elevation in V4R has a sensitivity of 88%, specificity of 78% and diagnostic accuracy of 83% in the diagnosis of RV MI. [see Inferior STEMI]
V4R ECG lead placement
Erhardt et al first described the use of a right sided precordial lead (CR4R or V4R) in the diagnosis of right ventricular infarction which had previously been thought to be electrocardiographically silent. [Single right-sided precordial lead in the diagnosis of right ventricular involvement in inferior myocardial infarction. Am Heart J. 1976]
Posterior leads
Leads V7-9 are placed on the posterior chest wall in the following positions:
- V7 – Left posterior axillary line, in the same horizontal plane as V6.
- V8 – Tip of the left scapula, in the same horizontal plane as V6.
- V9 – Left paraspinal region, in the same horizontal plane as V6.
See Posterior STEMI

Lewis lead (S5-lead)
The Lewis lead configuration can help to detect atrial activity and its relationship to ventricular activity. Named after Welsh cardiologist Sir Thomas Lewis (1881-1945) who first described in 1913. Useful in:
- Observing flutter waves in atrial flutter
- Detecting P waves in wide complex tachyarrhythmia to identify atrioventricular dissociation
Lewis lead placement
- Right Arm (RA) electrode on manubrium
- Left Arm (LA) electrode over 5th ICS, right sternal border.
- Left Leg (LL) electrode over right lower costal margin.
- Monitor Lead I
Original Lewis Lead description (1913)
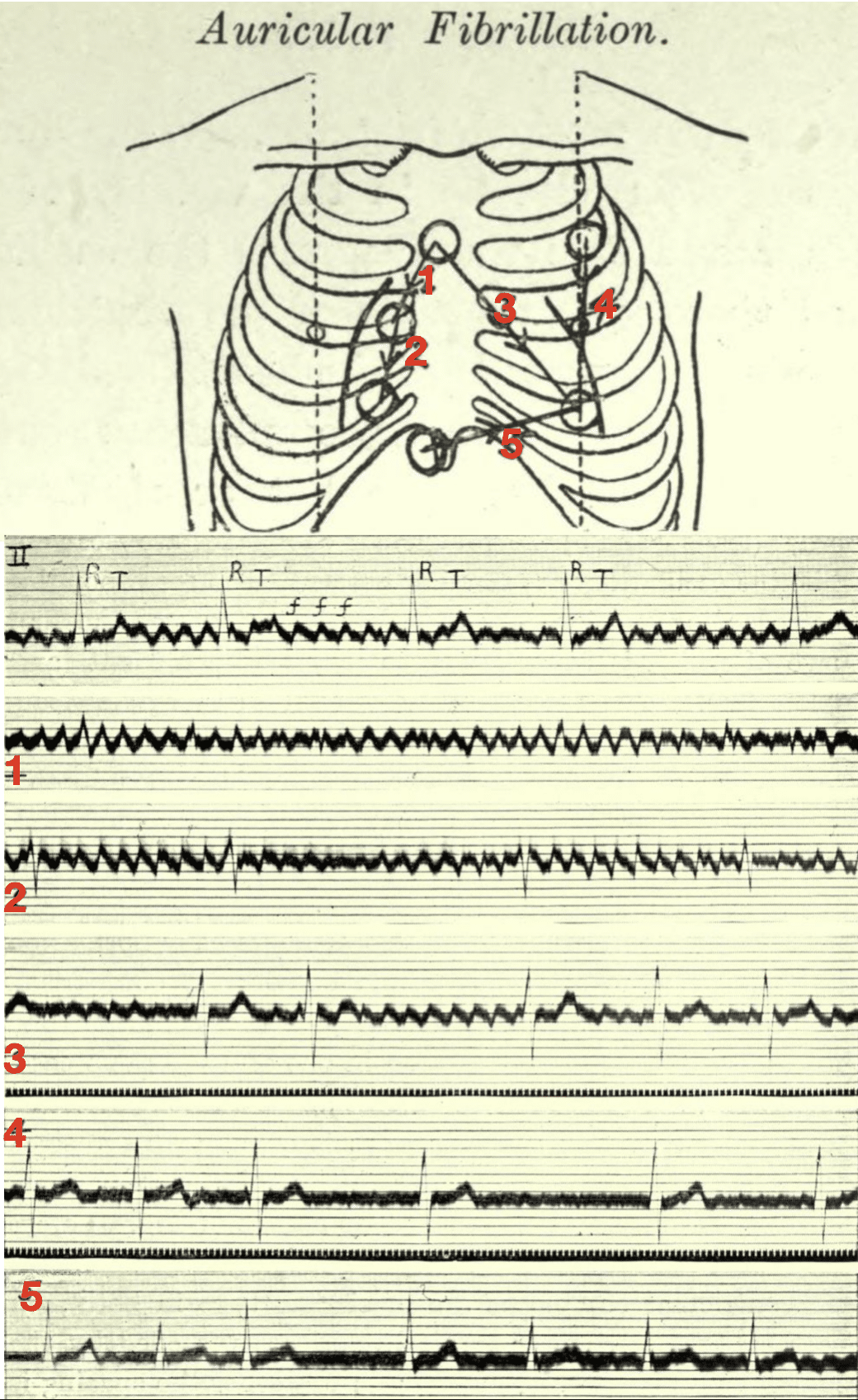
Thomas Lewis developed and described (1913) his lead configuration to magnify atrial oscillations present during atrial fibrillation.
When fibrillation is present and the electrodes lie in the vicinity of the right auricle (leads 1 and 2 of the diagram) the oscillations are maximal, and there is but a trace of the ventricular beats. When they lie in the long axis of the heart (lead 3) then both the oscillations and the ventricular complexes are conspicuous. Finally, when they lie along the left or right ventricular border (leads 4 and 5) the ventricular complexes are clear cut while the oscillations are small or absent.
The corresponding electrocardiograms are shown below the diagram, the first curve of which is from the customary lead II (right arm to left leg). The oscillations of fibrillation are readily identified in this manner and their origin in the auricle is clearly indicated. In tremulous subjects, no oscillations are seen in any of the special leads.
Lewis 1913
Lewis T. Auricular fibrillation 1913
The first electrocardiogram is from lead II; it consists of irregularly placed ventricular complexes (R, T) and of large and continuous oscillations (f f).
The remaining five curves are from the chest wall.
- 1 and 2 were taken from the area overlying the right auricle; in these leads the oscillations are maximal and the ventricular complexes are minimal.
- 3 was taken from an oblique lead covering the whole heart, and it shows both oscillations and ventricular complexes.
- 4 and 5 were taken from leads along the margins of the ventricles; they show but little sign of the oscillations.
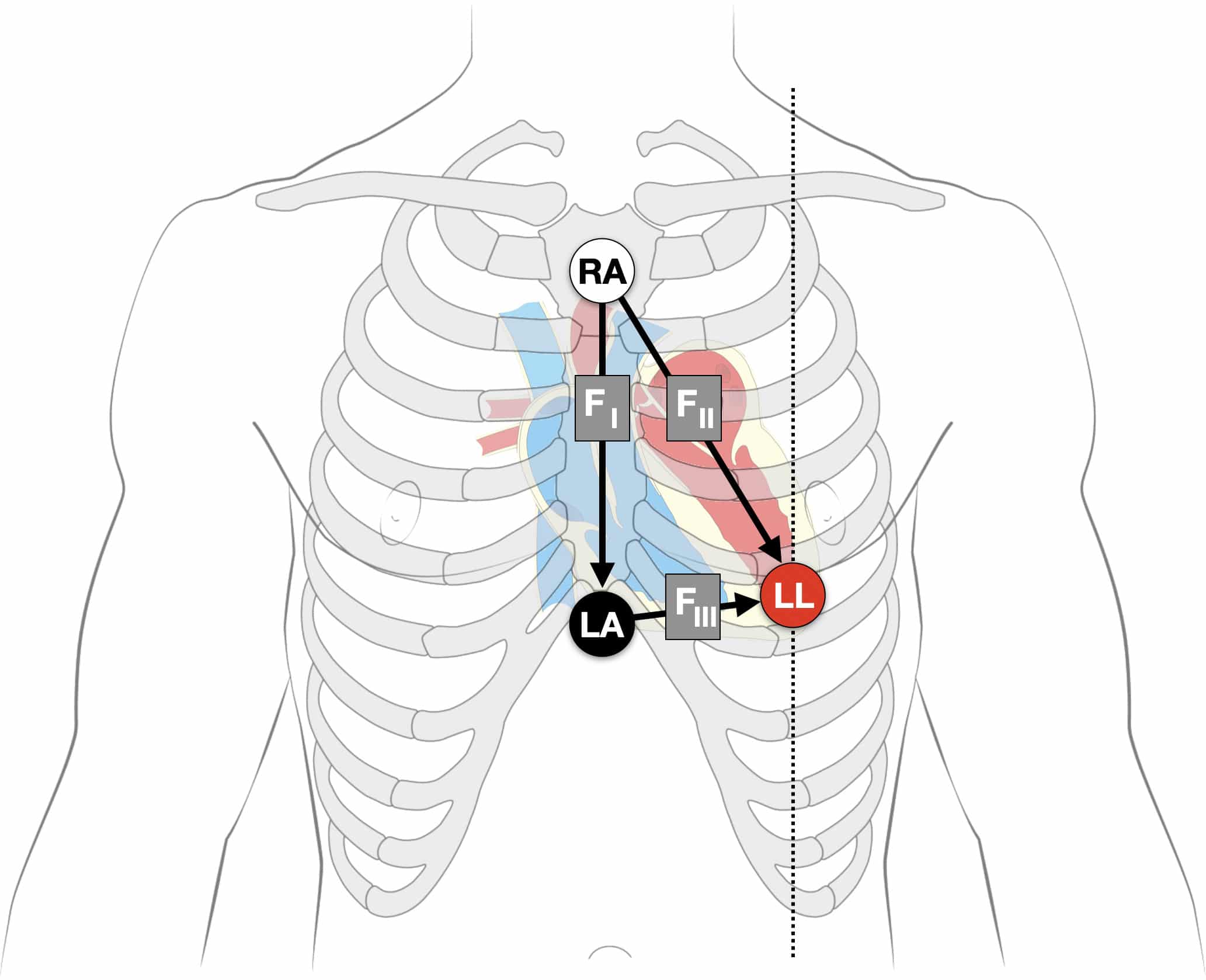
Fontaine leads
Fontaine bipolar precordial leads (F-ECG) are used to increase the sensitivity of epsilon wave detection. Named after French cardiologist and electrophysiolgist Guy Hugues Fontaine (1936-2018). Leads are placed as shown:
- Right Arm (RA) over the manubrium;
- Left Arm (LA) over the xiphoid process;
- and Left Leg (LL) in the standard V4 position (5th ICS MCL).
Instead of regular leads I, II, and III there are now three bipolar chest leads that are termed FI, FII, and FIII which record the potentials developed in the right ventricle, from the infundibulum to the diaphragm.
The vertical bipolar lead FI, (similar to aVF) magnifies the atrial potentials and can be used to record:
- epsilon waves;
- search for AV dissociation in ventricular tachycardia;
- and to study abnormal atrial rhythms when the P waves are too small on regular leads.
ECG Electrode Guide
ECG Academy Videos
The ECG Lead
The Limb Leads
The Precordial Leads
Related Topics
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
What is the point of moving the LL limb lead for monitoring the Lewis Lead, if we’re only monitoring lead I? It’s my understanding that the only leads being used by the machine in Lead I is RA, LA, and ground (RL).
Monitoring in lead 1 with the Lewis lead position looks through the right atrium closer to the sternal edge. Moving the LL out and lower gives another view through the right atrium to support what is seen in lead 1. This is because the RA lead position is changed and the new placement of the LA and LL now allow us to look through the Right atrium more closely.
Great article. Question- 15-lead ECGs- here in NC there a trend of acquiring a 15-lead ECG, which essentially just moves V4, V5, and V6 to the other side of the chest. How valuable would this be as opposed to a right sided ECG using V3, V4, V5, and V6 on the right?
Can I just mention how much you and healio.com have saved my life and my medical career???
[…] fantastic description of these is available HERE and in Chapter 7 of Prof Peate’s pathophysiology […]