
![]()
ECG Case 109
84 year old male presents complaining of general lethargy, nausea, several episodes of diarrhea, and dizziness. Past history of atrial fibrillation, diabetes, and hypertension.
Medications include aspirin, ACE inhibitor, statin, sulphonylurea, and digoxin.
He is conscious, vague but orientated, and his BP is 112 systolic.
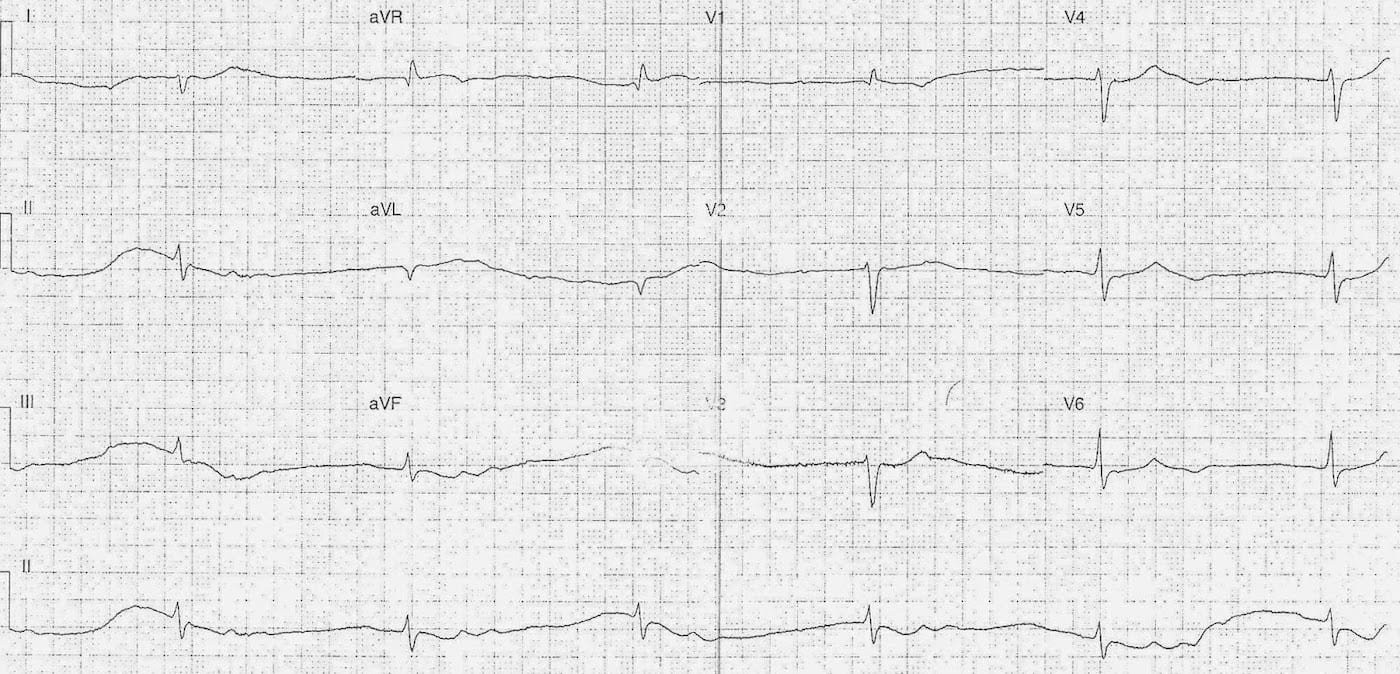
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Rate:
- 36
Rhythm:
- Regular
- Nil p waves visualised
Axis:
- RAD (~160 deg)
Intervals:
- PR – nil p waves
- QRS – Prolonged (120-130ms)
- QT – 550ms
Segments:
- Wandering baseline makes assessment difficult
- ? Minor ST depression III, aVF, V5-6
Additional:
- U waves
- Best visualised lead II
- Secondary to digoxin toxicity
Interpretation:
- “Regularised AF”
- Escape rhythm – likely junctional as QRS morphology similar post Tx
- Atrial fibrillation
- 3rd Degree AV block
- QRS Prolongation
- likely secondary to hyperkalaemia
CLINICAL OUTCOME
What happened next?
Our patient is on digoxin with clinical features that whilst non-specific are often associated with chronic digoxin toxicity. As the comments section suggests digoxin toxicity should rate high on our list of likely diagnosis with associated electrolyte abnormalities.
Urgent electrolytes and digoxin levels were performed and this patient had a digoxin level of 5.4 ng/ml and a potassium > 9.0 !
He was treated with digoxin immune Fab, following which a repeat ECG was performed.

The ECG following treatment shows rate controlled atrial fibrillation (~66bpm), normalisation of QRS width (80-100ms), and decreased prominence of the U waves.
CLINICAL PEARLS
Chronic Digoxin Toxicity
I like to just focus on ECGs with this blog but I thought we’d just touch on one of the unique features of chronic digoxin toxicity which is hyperkalaemia and “stone heart”.
Hyperkalaemia, digoxin toxicity, and calcium therapy – ‘Stone Heart’
Stone heart refers to life-threatening cardiac tetany due to the use of i.v. calcium to treat hyperkalaemia in the setting of digoxin toxicity.
The theory being:
- Digoxin works by inhibiting cardiac sodium-potassium ATPase pump
- This increases intracellular sodium and calcium in the cardiac myocyte
- Increased intracellular calcium = increased contractility and automaticity
- In toxic setting more calcium = cardiac tetany = irreversible contraction = death
First line treatment in chronic digoxin toxicity is Digoxin Immune Fab, a recommended empirical dose is 2 ampoules if features of toxicity, and 5 ampoules in the setting of cardiac arrest in which chronic digoxin toxicity is suspected. In the absence of Fab or as adjuncts to treat hyperkalaemia options include sodium bicarb, insulin / dextrose, and magnesium sulphate.
The Toxicology Handbook, which is a must own textbook for anyone doing Emergency Medicine and certainly the most useful EM book I own, states calcium is contraindicated in treating hyperkalaemia in the setting of digoxin toxicity. This is echoed by a number of other sources such as, this letter in the EMJ, and the eMedicine review of the emergency management of digoxin toxicity.
There is certainly an amount of debate as to the existence of the ‘Stone Heart’ and the danger of using calcium in the setting of digoxin related hyperkalaemia. I’m not going to go through this here as a number of other people have covered the topic more eloquently than I could, I will just link to some further readings below:
- Levine M, Nikkanen H, Pallin DJ.The effects of intravenous calcium in patients with digoxin toxicity. J Emerg Med. 2011 Jan;40(1):41-6.
- CCC – Calcium, Digoxin Toxicity and Stone Heart Theory
- TPR – Heart of Stone ? Calcium & Digoxin Toxicity
- EPMonthly – “Stone Heart” = Stone Ages?
- ECG Library – Digoxin Toxicity
- CCC – Digoxin Toxicity
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |
How can you say that its 3rd degree AV block if no P waves?
Apparently , it looks there are P waves in rythem leads not associated with QRS complexes .