
![]()
ECG Case 110
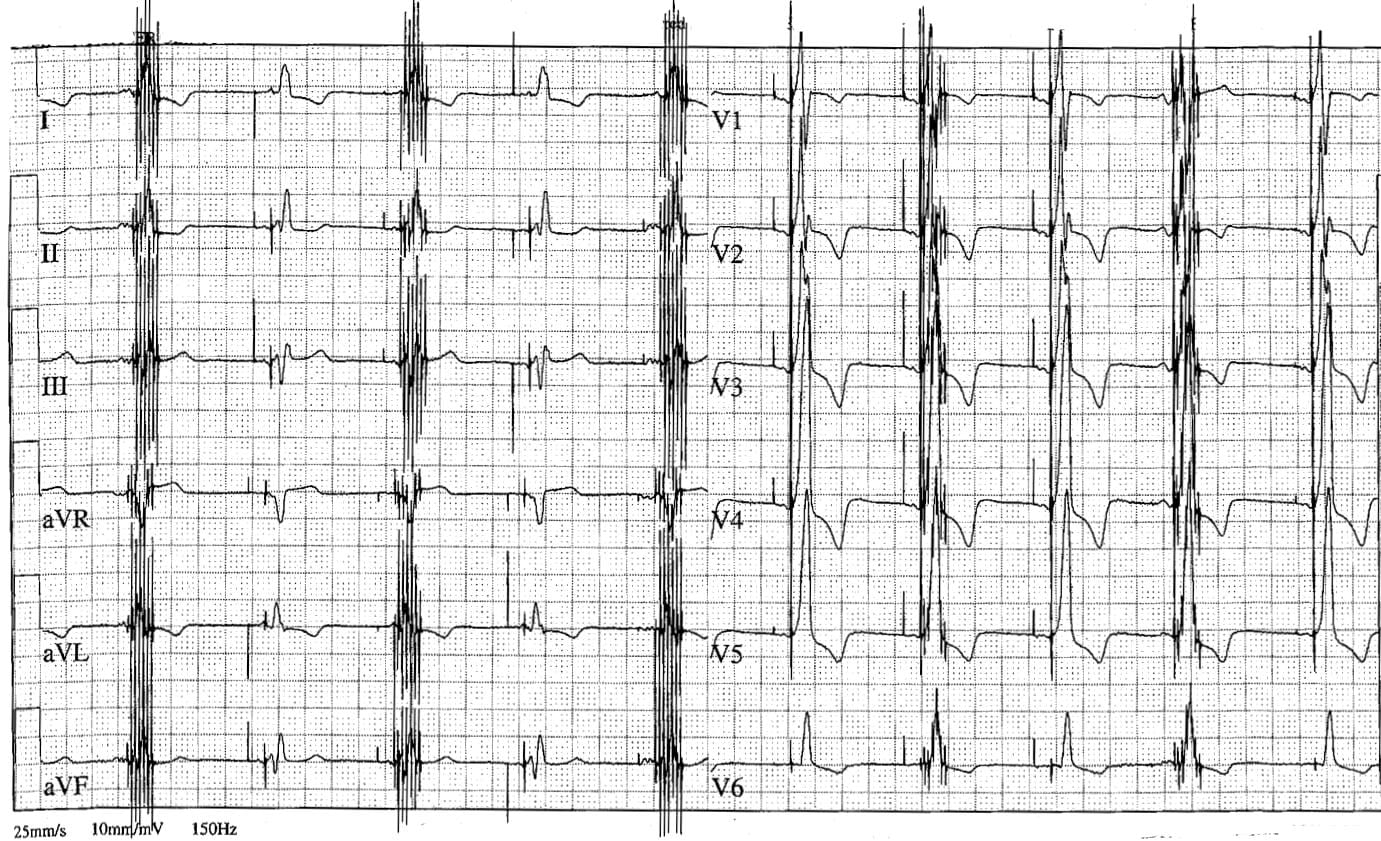
This ECG is from a middle aged female with a history of cardiac failure.
Describe and interpret this ECG
ECG REVIEW
Rate:
- 60
Rhythm:
- Regular
- Paced rhythm
- A-V Sequential pacing
- All complexes paced
Axis:
- Normal (~30 deg)
Intervals:
- QRS – Prolonged (160ms)
- QT – 460ms
Segments:
- ST Depression Leads I, II, aVL, V1-6
- Discordant to QRS vector
Additional:
- T wave inversion leads I, aVL, V1-6
- Discordant to QRS vector
- Dominant R wave in V1
- High frequency signal
- Occurs at every alternate QRS complex
- Does not occur at any other points during ECG recording
Note: ECG kindly donated by Dr A Keren, a consultant cardiologist and cardiac electrophysiologist.
ECG INTERPRETATION
So what’s going on here?
Let’s start with the easiest bit of the ECG.
We’ve got a paced rhythm with the following features:
- A-V sequential pacing
- Dominant R wave V1
- ST and T wave changes discordant to QRS vector
What does this mean ?
The dominant R wave in lead V1 and a Rsr’ pattern in lead V2 signifies left ventricular dominant biventricular pacing, commonly referred to as Cardiac Resynchronisation Therapy (CRT).
In CRT pacing leads are placed in the right ventricle, right atrium, and a coronary sinus branch (preferable posterior / posterolateral location). The purpose of CRT is restore the synchronous beating of right and left ventricle, as dyssynchronous ventricular contraction can impair pump function.
- Barold SS, Herweg B. Usefulness of the 12-lead electrocardiogram in the follow up of patients with cardiac resynchronization devices. Part I. Cardiol J. 2011;18(5):476-86.
- Barold SS, Herweg B. Usefulness of the 12-lead electrocardiogram in the follow up of patients with cardiac resynchronization devices. Part II. Cardiol J. 2011;18(6):610-24.
- Burkhardt JD, Wilkoff BL. Interventional electrophysiology and cardiac resynchronization therapy: delivering electrical therapies for heart failure. Circulation. 2007 Apr 24;115(16):2208-20
- Leclercq C. Problems and troubleshooting in regular follow-up of patients with cardiac resynchronization therapy. Europace. 2009 Nov;11 Suppl 5:v66-71.
What about the other signal ?
As noted above the most striking feature of this ECG is the high frequency signal overlying every alternate QRS.
Other possibilities include nerve stimulator sources, TENs source, or pacemaker failure.
The patient had a Cardiomyoplasty procedure for severe heart failure. Skeletal muscle is wrapped around the heart and connected to a high frequency pacemaker which is also connected to the heart in order to trigger the pacemaker. Skeletal muscle is used to increase ejection fraction but is not the same as cardiac muscle. It is hard to make skeletal muscle have a full contraction just with one pacing spike as we do for pacing the heart. To make skeletal muscle contract you need to give it sustained high frequency contraction which in this patient was programmed for every second beat. If you made it every beat, the skeletal muscle would fatigue and be ineffective.
You can read more about cardiomyoplasty in this nice review article by Bocchi, link below:
- Bocchi EA. Cardiomyoplasty for treatment of heart failure. Eur J Heart Fail. 2001 Aug;3(4):403-6
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |
both 1st and 9th p wave may be patient’s own (nate) p wave