
![]()
ECG Case 111
ECG is from a 69 year old male who had a dual chamber pacemaker inserted earlier in the day. He complained to the ward staff of pain at the insertion site and you’ve been asked to review him. His BP, temp, sats, resp rate are all within normal limits.
An ECG and CXR are performed, results below.
Describe and interpret this ECG and CXR
ECG ANSWER and INTERPRETATION
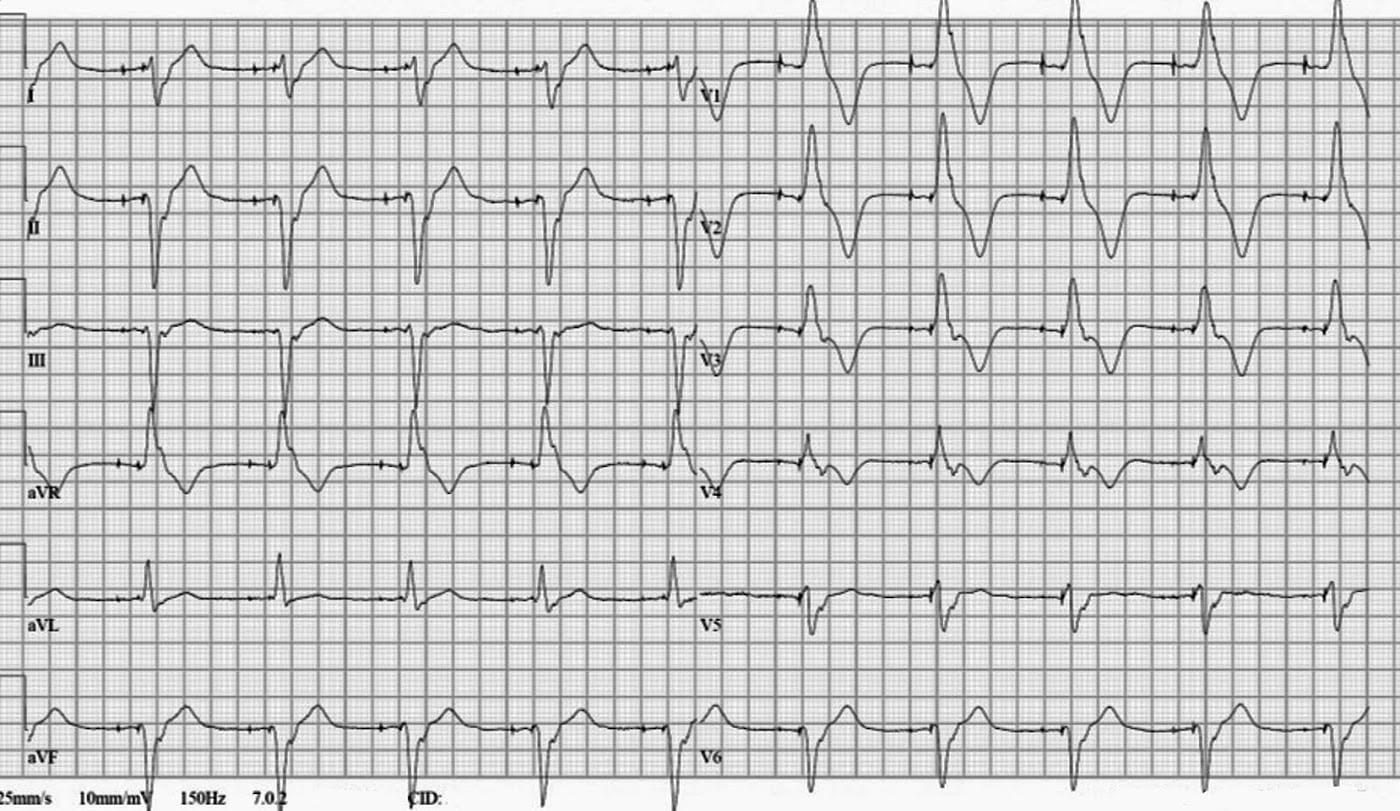
Rate:
- 60
Rhythm:
- Regular
- A-V Sequential pacing
Axis:
- Extreme / NW axis (-110 deg)
Intervals:
- QRS – Prolonged (180ms)
- QT – 480ms
Segments:
- ST elevation leads I, II, V6
- Discordant to QRS vector
- ST depression leads aVR, V1-4
- Discordant to QRS vector
Additional:
- T wave inversion leads aVR, V1-4
- Discordant to QRS vector
- RBBB Morphology
Interpretation:
- A-V Sequential pacing with capture
- RBBB Morphology in ventricular paced complexes
- This is NOT what we would expect to see.
Note: right ventricular pacing should result in a LBBB morphology, with left ventricular pacing causing an RBBB morphology
This ECG should raise the concern of inappropriate lead placement with resultant left ventricular pacing. Lead misplacement could be due to passage of lead through a PFO, ASD or VSD, septal perforation, or coronary sinus lead placement.
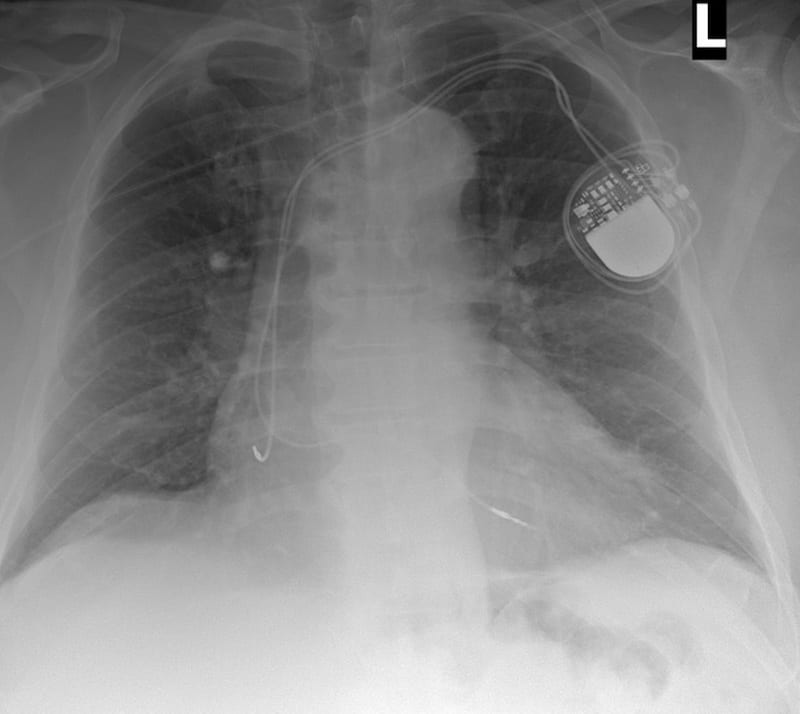
PA CXR INTERPRETATION
PA chest x-ray with appropriate penetration, exposure, with some rotation.
A dual chamber pacemaker is in-situ with atrial and ventricular leads noted, it is possible the ventricular lead crosses high, but overall position looks OK.
The right costophrenic angle is not fully visualised, but the left costophrenic angle is clear.
There is cardiomegaly with the cardiothoracic ratio ~0.6.
There is no visible pneumothorax.
There is an oblique artefact across the upper thorax likely either oxygen tubing or monitoring cable.
But we’re concerned about the lead position given our ECG findings and the PA CXR hasn’t really helped…
FURTHER IMAGING
…so how about a lateral CXR?

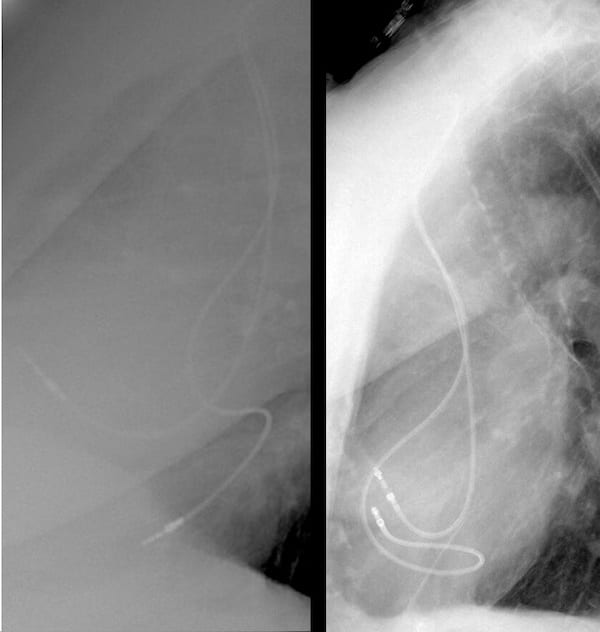
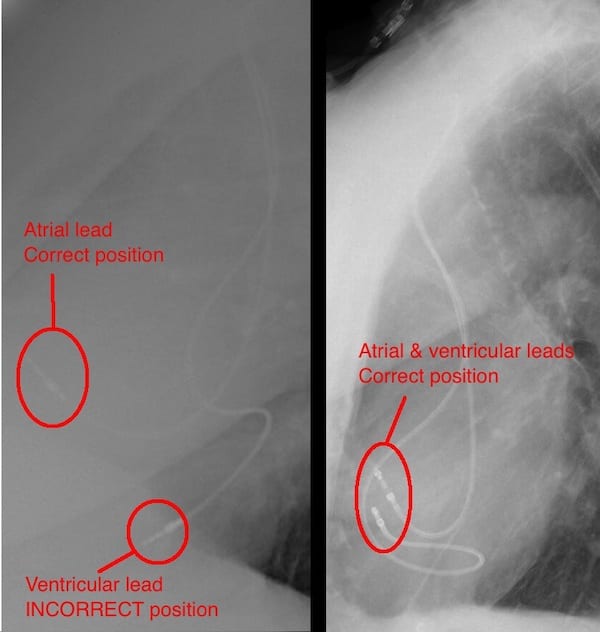
Lat CXR Post PPM Lat CXR Post PPM labelled


For many of us the role of the lateral CXR is to localise or investigated pulmonary pathology, and we don’t always look at the cardiac silhouette. In this case an understanding of the lateral cardiac silhouette is essential to confirm our ECG suspected diagnosis.
Looking at this lateral CXR we can see one pacemaker lead sits anteriorly, and the other is sitting posteriorly, this is NOT normal.
On a lateral CXR the right ventricle sits anteriorly with the left ventricle sitting posteriorly.
This CXR confirms ventricular lead placement in the left ventricle.
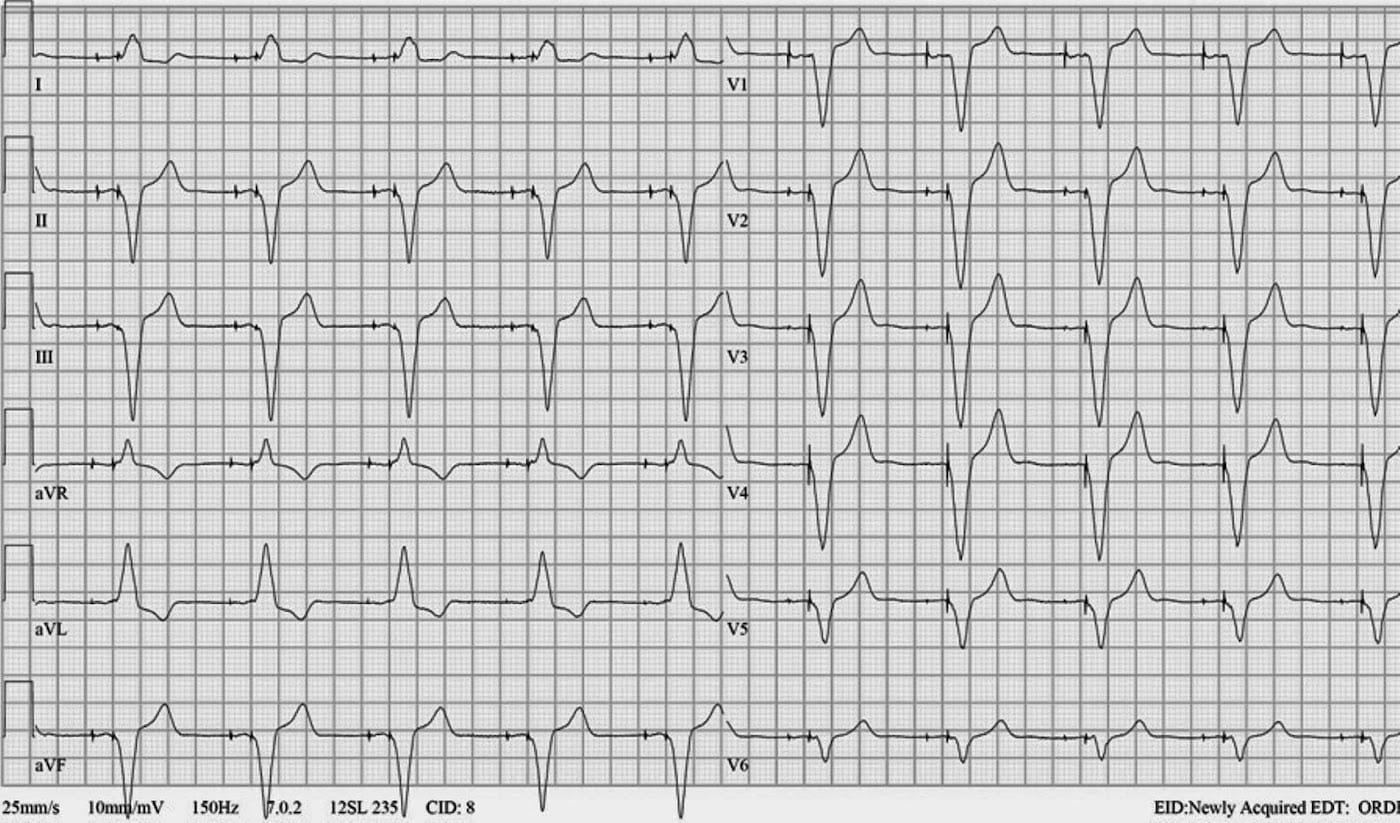
CLINICAL OUTCOME
In this case the lead had passed through a PFO, through the mitral valve, and was sitting in the left ventricle !
The ECG below is following lead repositioning with correct right ventricular placement. Note the change in QRS morphology compared with previous, this ECG shows the LBBB pattern consistent with appropriate right ventricular lead placement.
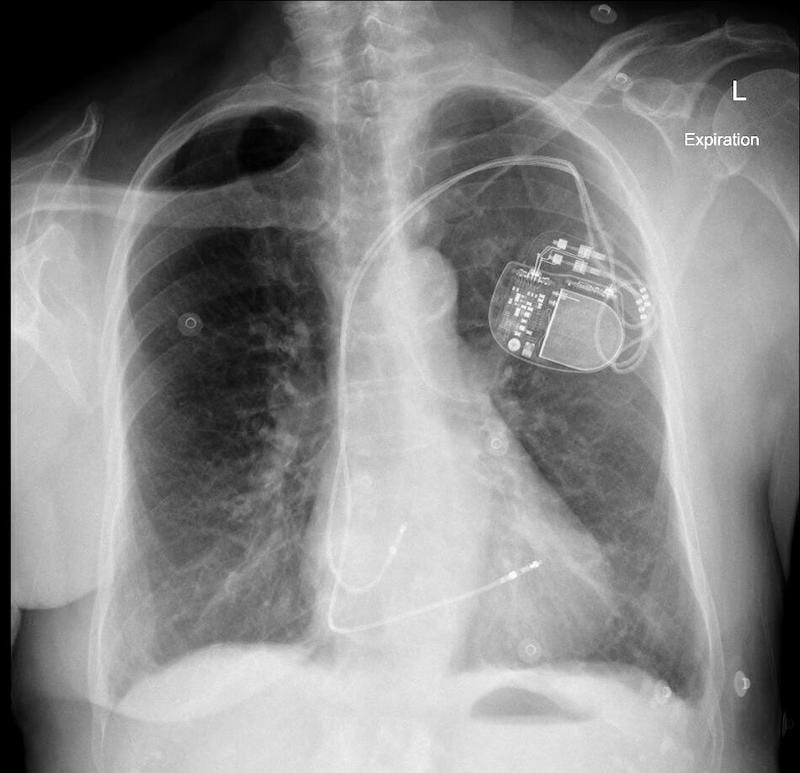
Normal PPM Lead Placement CXR
The following PA and lateral CXR are taken from an unrelated case with appropriately placed pacing leads in the right atrium and right ventricle.
- Note the PA CXR appearance is not too different from the PA CXR in our case of lead misplacement
- Note on the lateral CXR both leads are placed anteriorly signifying right sided placement.
- Side-by-side comparison of cardiac silhouettes. Abnormal on left. Normal on right.

AP CXR PPM Normal 
Lat CXR PPM Normal 
Comparison of cardiac silhouettes – Abnormal on left. Normal on right. Lat cardiac comparison labelled

Is RBBB morphology during right ventricular pacing always due to lead malposition?
The short answer to this is no.
There are cases in which an RBBB morphology can occur with appropriate right ventricular apical pacing.
Features which may assist in differentiating between lead malposition and correct placement include:
- Frontal plane axis
- Precordial transition point
- Repositioning of leads V1-2
I would recommend the following freely available papers which both include a review of RBBB morphology during right ventricular pacing.
- Erdogan O, Aksu F. Right bundle branch block pattern during right ventricular permanent pacing: Is it safe or not? Indian Pacing Electrophysiol J. 2007 Aug 1;7(3):187-91
- Almehairi M, Baranchuk. Right Bundle Branch Block Morphology During Apical Right Ventricular Pacing. The Journal of Innovations in Cardiac Rhythm Management, 4 (2013), 1303–1304.
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |
good explanation! Thank you so much for this! Very useful.
Keep them coming! 😻
Absolutely exceptional!! Congratulations for all the work you do in order for us to have access to these amazing cases!!!