
![]()
ECG Case 115
The following ECG is from a 71yr old male who presented with several episodes of ischaemic sounding chest pain on a background of known ischaemic cardiac disease.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
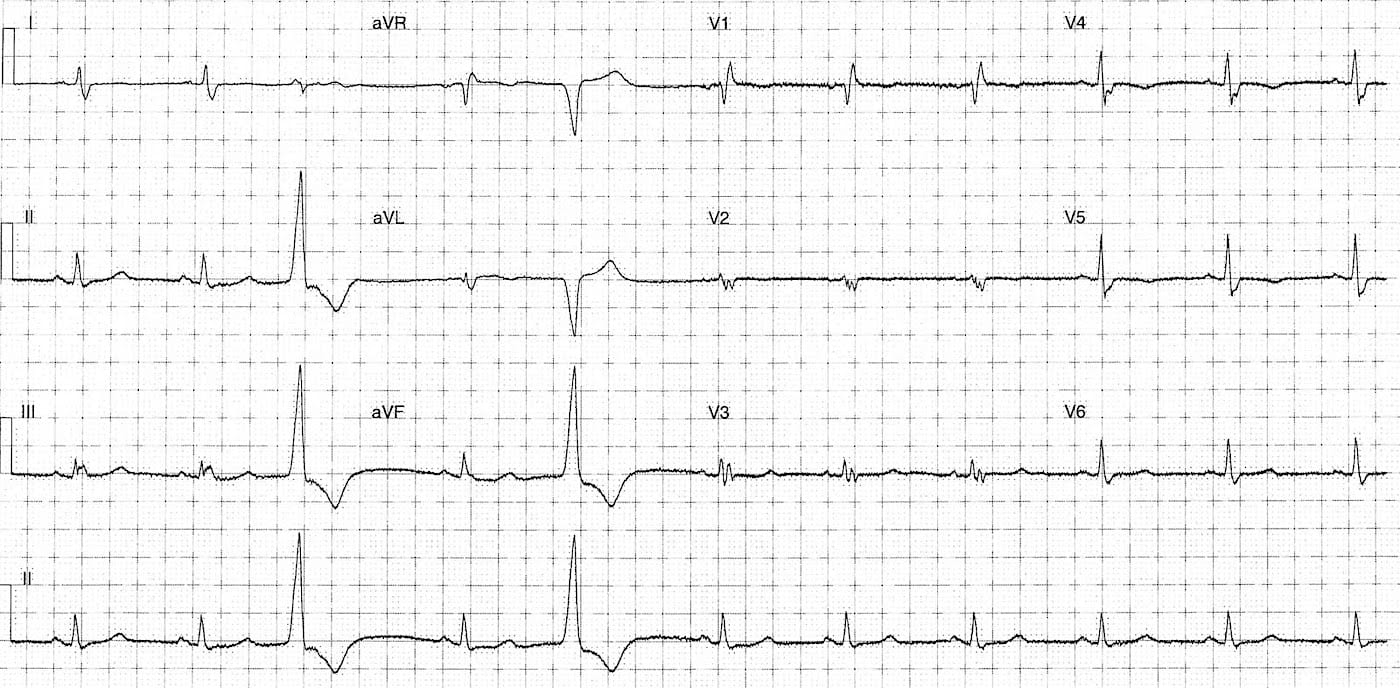
Rate:
- Mean rate 66 bpm
Rhythm:
- Sinus rhythm
- Unifocal PVCs
Axis:
- Normal
Intervals:
- PR – Normal (~200ms)
- QRS – Prolonged (120-130 ms)
- QT – 410ms (QTc Bazett 470 ms)
Additional:
- QRS fragmentation
- Best seen leads V2-3
- Lead V2 rsr’s’r”s” pattern
- Lead V3 rsr’s’ pattern
- T wave inversion leads V4-5
- ST elevation leads aVR and aVL (< 1mm)<1mm font=””>
- ST depression leads II, III, aVF
Interpretation:
- ST and T wave changes
- Likely ACS given history
- Needs serial ECGs and comparison with prior ECGs
- QRS Fragmentation
- Caused by abnormal ventricular repolarisation
- Due to myocardial scarring, fibrosis or ischaemia
CLINICAL OUTCOME
QRS Fragmentation
The two following papers are a great overview of QRS fragmentation including diagnostic morphology and clinical relevance in terms of associations and effects on morbidity and mortality.
Further reading:
- Jain R, Singh R, Yamini S, Das MK. Fragmented ECG as a Risk Marker in Cardiovascular Diseases. Curr Cardiol Rev. 2014; 10(3): 277–286.
- Mittal SR. Fragmented QRS: A simple electrocardiographic prognostic marker in cardiovascular disease. J Clin Prev Cardiol 2016; 5: 94-8
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |
