
![]()
ECG Case 114
20 yr old female who presented to the Emergency Department following an episode of chest pain. At review she was pain free and all vital signs were normal. Her serial ECG’s are below, there is ~30 mins between each ECG.
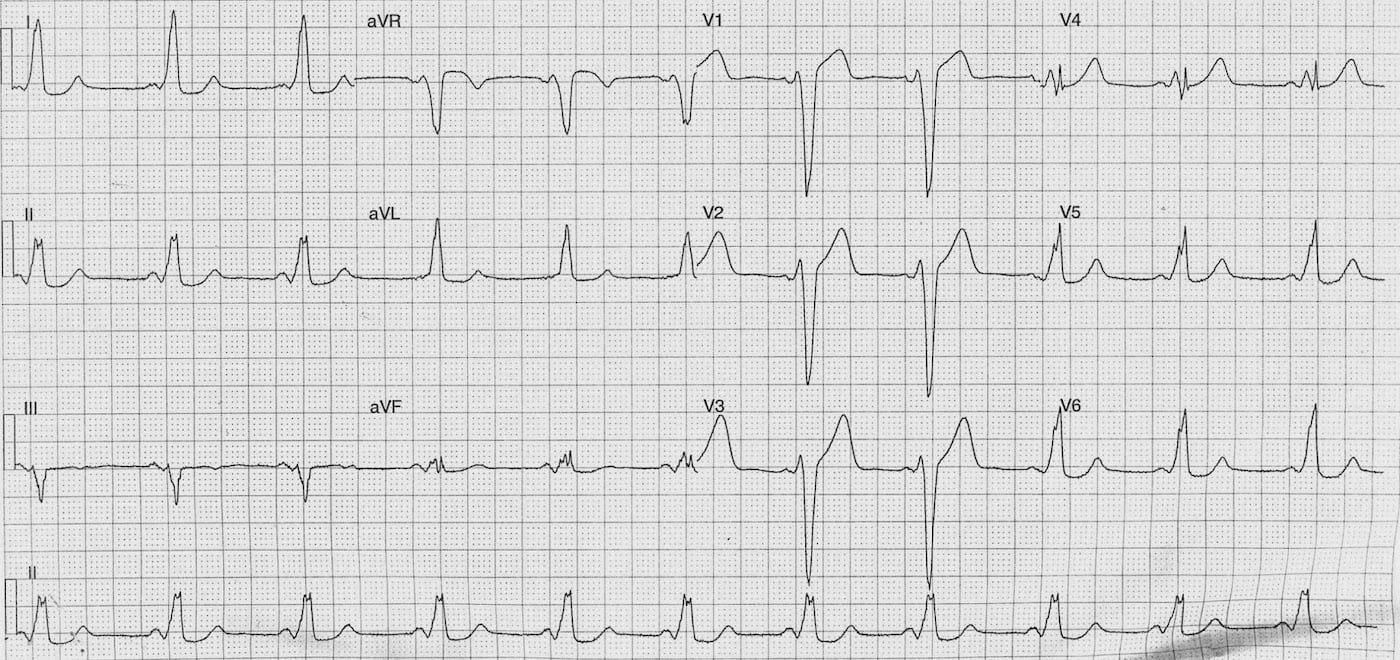
Describe and interpret ECG 1
ECG ANSWER and INTERPRETATION
Rate:
- ~66 bpm
Rhythm:
- Regular
- Sinus rhythm
Axis:
- Normal
Intervals:
- PR – Short (100ms)
- QRS – Prolonged (140-160 ms)
- QT – 440ms (QTc Bazett 460 ms)
Segments:
- ST Elevation lead avR
- ST Depression leads I, II, aVL, aVF, V5-6
Additional:
- T wave inversion lead III
- Delta waves best seen in lateral precordial leads
Interpretation:
- Wolff-Parkinson-White
- Type B Pattern
- AP location right posterior or postero-lateral – thanks Adrian 🙂
- The QRS prolongation, QRS morphology and ST segment changes are all due to pre-excitation.
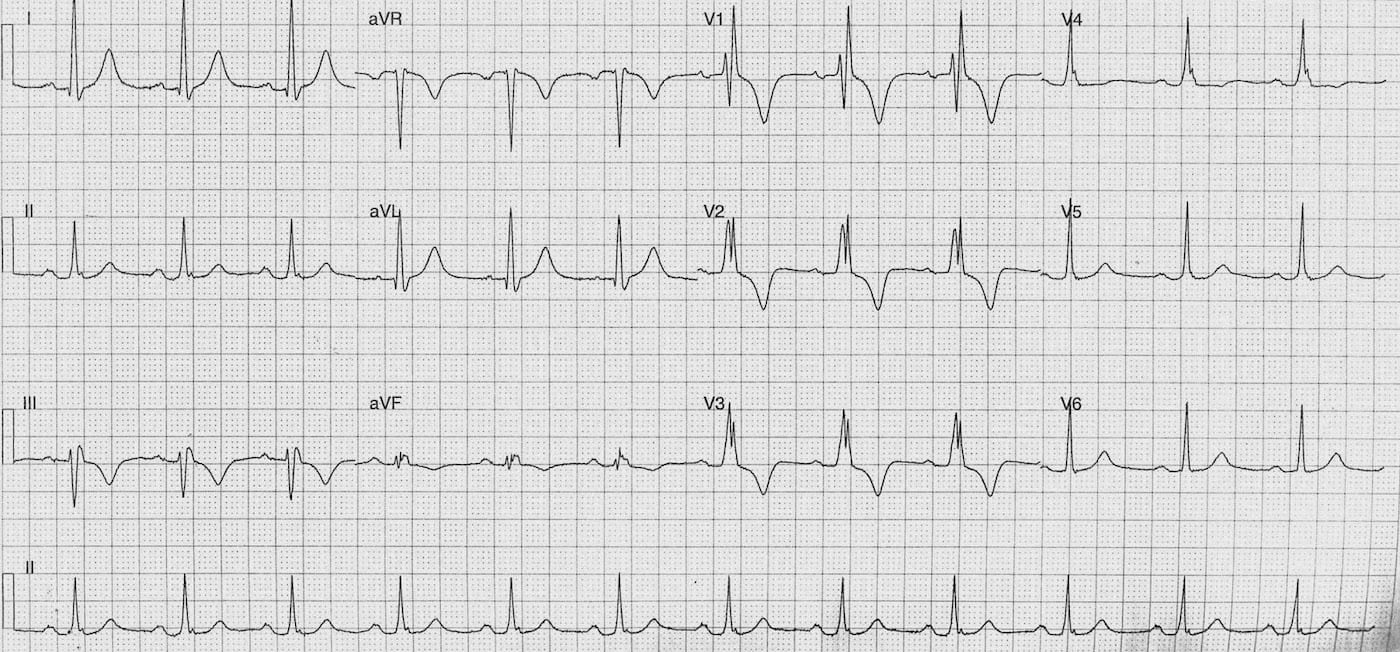
Describe and interpret ECG 2
ECG ANSWER and INTERPRETATION
Rate:
- ~72 bpm
Rhythm:
- Regular
- Sinus rhythm
Axis:
- Normal
Intervals:
- PR – Normal (~200ms)
- QRS – Prolonged (120ms)
- QT – 360ms (QTc Bazett 395 ms)
Additional:
- RBBB Pattern
- Deep T inversion leads III, V1-3
Interpretation:
- Loss of accessory pathway conduction
- Resolution of pre-excitation features
- PR now normal
- QRS narrower
- No delta waves
- Change in QRS morphology
CLINICAL OUTCOME
But what about the T waves ?
The most striking thing to my eye regarding the second ECG is the relative depth of the T-waves. They look deeper than one would expect from the RBBB alone.
There is a very broad range of potential causes of such T-wave changes including ischaemia, cardiomyopathy, myocarditis, raised ICP, PE and hyperventilation.
There is also another cause of T-wave change that is very likely in this case which is ‘Cardiac T-wave memory’ this occurs after a period of abnormal ventricular depolarisation e.g. paced rhythm, VT, SVT with aberrancy and preexcitation.
Vakil et al provide a nice overview of T-wave memory, proposed mechanisms, and a case example.
The deep T wave inversion on this ECG correspond to the leads in which a negative QRS was seen in the patients pre-excited ECG. Patient’s often require work-up to exclude underlying ischaemia or structural disease but cardiac T-wave memory is a benign and self-resolving condition in itself.
What happened ?
Well our patient had a negative troponin and D-dimer with a normal chest x-ray. Her pain was felt to be benign in origin. She was reviewed by cardiology in light of her pre-excitation and out-patient follow-up arranged.
REFERENCES
LITFL references
- ECG Case 106 (Cardiac T-wave memory)
- ECG Library – Right Bundle Branch Block RBBB
- ECG Library – Pre-excitation syndromes
References on Cardiac T-wave memory
- Vakil K, Gandhi S, Abidi KS, et al. Deep T-Wave Inversions: Cardiac Ischemia or Memory? JCvD 2014;2(2):116-118
- Folco EJ, Roder K, Mitchell GF, Koren G. “Cardiac memory”: a struggle against forgetting. Circ Res. 2003 Sep 5;93(5):384-6.
- Ghosh S, Rhee EK, Avari JN, Woodard PK, Rudy Y. Cardiac Memory in WPW Patients: Noninvasive Imaging of Activation and Repolarization Before and After Catheter Ablation. Circulation. 2008 Aug 26;118(9):907-15.
- Chiale PA et al. The multiple electrocardiographic manifestations of ventricular repolarization memory. Curr Cardiol Rev. 2014 Aug;10(3):190-201.
- Ali FS, Baranchuk A. Cardiac Memory Variations in Surface ECG Precordial Mapping. The Journal of Innovations in Cardiac Rhythm Management (JICRM). 2014
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |
For this ECG, I was under the impression that V1, V2, V3 showed ST-elevation in ECG 1? Could anyone explain why this was not the case?
ST-elevation is present, but is typical of WPW.
IN ECG 1 LBBB Pattern is present ( wide QRS + M pattern (rsr prime) in V5 and V6 and deep S wave in V1 and V2) !!
True! And I think that left atrial enlargement are present too